
Abstract
Background Multiple COVID-19 outbreaks have occurred in homeless shelters across the US, highlighting an urgent need to identify the most effective infection control strategy to prevent future outbreaks.
Methods We developed a microsimulation model of SARS-CoV-2 transmission in a homeless shelter and calibrated it to data from cross-sectional polymerase-chain-reaction (PCR) surveys conducted during COVID-19 outbreaks in five shelters in three US cities from March 28 to April 10, 2020. We estimated the probability of averting a COVID-19 outbreak in a representative homeless shelter of 250 residents and 50 staff over 30 days under different infection control strategies, including daily symptom-based screening, twice-weekly PCR testing and universal mask wearing.
Results The proportion of PCR-positive residents and staff at the shelters with observed outbreaks ranged from 2.6% to 51.6%, which translated to basic reproduction number (R0) estimates of 2.9−6.2. The probability of averting an outbreak diminished with higher transmissibility (R0) within the simulated shelter and increasing incidence in the local community. With moderate community incidence (∼30 confirmed cases/1,000,000 people/day), the estimated probabilities of averting an outbreak in a low-risk (R0=1.5), moderate-risk (R0=2.9), and high-risk (R0=6.2) shelter were, respectively: 0.33, 0.11 and 0.03 for daily symptom-based screening; 0.52, 0.27, and 0.04 for twice-weekly PCR testing; 0.47, 0.20 and 0.06 for universal masking; and 0.68, 0.40 and 0.08 for these strategies combined.
Conclusions In high-risk homeless shelter environments and locations with high community incidence of COVID-19, even intensive infection control strategies (incorporating daily symptom-screening, frequent PCR testing and universal mask wearing) are unlikely to prevent outbreaks, suggesting a need for non-congregate housing arrangements for people experiencing homelessness. In lower-risk environments, combined interventions should be adopted to reduce outbreak risk.
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) poses great risk to people experiencing homelessness. Across the United States (US), the estimated 568,000 people who experience homelessness nightly (1) are likely to suffer a disproportionate disease burden and need for hospitalization (2,3). People experiencing homelessness are on average older and have a high prevalence of comorbidities that are risk factors for severe COVID-19 (2). Multiple outbreaks in homeless shelters have occurred in several cities including San Francisco, Boston, Seattle and Atlanta with attack rates of up to 67% (4–7). Homeless shelters have had to remain open in most cities despite high incidence of infection in the community, concern about the risk of further outbreaks, and uncertainty over the effectiveness of different infection control strategies. There is an immediate need to identify the best infection control strategy to reduce the risk of outbreaks and assess the safety of continuing to operate congregate shelters where transmission in the community is high.
The role of shelters and associated infection control practices in transmission of COVID-19 among people experiencing homelessness is still poorly understood. Given current understanding that SARS-CoV-2 virus is transmitted predominantly through respiratory droplets, with some airborne and fomite transmission (8), there is a need to consider policies to limit transmission within high-density congregate living environments. Different infection control strategies are currently recommended based on the level of transmission in the external community (9). These include routine symptom screening, polymerase chain reaction (PCR) testing, universal mask wearing, and relocation of individuals at high risk of severe disease to non-congregate settings (10). There is limited evidence on the effectiveness of strategies to reduce transmission in congregate settings, and thus further research is urgently needed to guide city-level policy across the US.
The goal of this study is to identify the most effective infection control strategy to slow the spread of COVID-19 among people experiencing homelessness who reside in shelters. We address this pressing question by estimating comparative health outcomes of key infection control strategies using a simulation model calibrated to data on homeless shelter outbreaks.
Methods
Microsimulation model
We developed an individual-level stochastic susceptible-exposed-infectious-recovered (SEIR) model (11) to simulate transmission of SARS-CoV-2 in a congregate shelter population (Additional file 1: Figure S1). The model defines individuals as susceptible, exposed, infectious, or immune to SARS-CoV-2 (Additional file 1: Table S1). We constructed the model to include important aspects of the natural history of COVID-19, including sub-clinical infection, pre-symptomatic transmission, and age-specific differences in risk of severe symptoms. In the model, susceptible individuals become infected with SARS-CoV-2 at a rate proportional to the prevalence of infectious individuals inside the shelter and their infectiousness (assuming homogeneous mixing), plus a static force of infection based on the background infection incidence in the community outside the shelter. Upon infection, individuals enter a latent infection stage in which they incubate the virus but are not infectious. They then progress to become infectious and contribute to ongoing transmission. An age-dependent fraction of infected individuals develop clinical symptoms with associated risk of hospitalization and death (Additional file 1: Table S2), while the remainder have sub-clinical infection. Individuals who recover from infection are assumed to remain immune.
Data
The model was calibrated using aggregate data from PCR testing conducted during COVID-19 outbreaks in five shelters in three US cities − San Francisco (n=1), Boston (n=1) and Seattle (n=3) (4,6,7) − from March 28−April 10, 2020. We obtained de-identified individual-level data from the outbreak in the San Francisco shelter (see Additional file 1 and Additional file 1: Table S3 for details), which is fully described elsewhere (5). As of April 10, 2020, a total of 89 individuals (84 residents, 5 staff) of 175 tested (130 residents, 45 staff) in the shelter were PCR-positive. We obtained aggregate data from the outbreaks in the Boston and Seattle shelters, where identified COVID-19 cases triggered mass testing events (4,6,7). In the Boston shelter, 147 of 408 residents and 15 of 50 staff were PCR-positive during testing conducted April 2−3, 2020. The numbers of residents and staff tested and positive in the three Seattle shelters (shelters A, B and C) at two testing events conducted March 30−April 1 and April 7−8, 2020 are given in Additional file 1: Table S4. For the San Francisco shelter, we used daily census data to inform the shelter population size, which decayed over time, and risk stratification (Additional file 1: Figure S2). For the other shelters, we assumed a constant population size over time.
Model calibration
We calibrated the model to the aggregate numbers of individuals PCR-positive out of those tested in each shelter (daily data for the San Francisco shelter, cross-sectional for the Seattle and Boston shelters) using approximate Bayesian computation techniques (see Additional file 1). We fitted the following parameters: (i) the basic reproduction number R0 (the average number of secondary infections generated by the average infectious individual in an entirely susceptible shelter population), (ii) the number of latently infected individuals who initially entered the shelter E0, and (iii) the number of days before the first case was identified that these individuals entered the shelter D (Table 1). The remaining parameters were sourced from literature on natural history and epidemiology of SARS-CoV-2 (Table 1 and Additional file 1: Table S5).
Infection control strategies
We simulated six infection control strategies (Additional file 1: Table S6), selected via informal consultation with public health experts. 1) Daily symptom-based screening: daily screening of all individuals in the shelter involving a temperature and symptom survey. Individuals who screened positive were PCR tested, with 80% compliance, and isolated for 1 day pending the test result; if negative, they returned to the population. We used published data on the sensitivity of symptom-based screening with time since infection (12), which suggests that close to 100% of symptomatic cases (a subset of all true cases) would eventually be detected under repeated daily screening based on the definition of being symptomatic, even with low sensitivity of symptom screening on any one occasion (here assumed to be 40% to give a 98% probability of detection after 8 days of daily symptom screening). Despite reports of low specificity of symptom screening (13,14), a high specificity of 90% was assumed to prevent unrealistic levels of PCR testing and isolation of symptom-positive individuals awaiting test results. We assumed a minimum of 3 days between repeat PCR tests for the same individual based on typical clinical practice and test turnaround times. 2) Routine PCR testing: twice-weekly PCR testing of residents and staff based on prior literature analyzing reduction in transmission and cost-effectiveness under different testing frequencies (15–17). We assumed 75% sensitivity and 100% specificity of PCR testing based on published literature (18–21), a mean duration of detectable viral load (starting prior to development of symptoms) of 20 days (Additional file 1: Figure S3) (22–27), and 80% compliance with testing. We assumed test results were returned in 1 day, after which time individuals who tested PCR-positive were removed from the shelter population. 3) Universal mask wearing: wearing of surgical masks by all persons within the shelter. We assumed that surgical mask wearing reduced the amount of infectious SARS-CoV-2 material breathed into the air by infected individuals by 30% based on literature estimates from household studies assuming high compliance and recent experimental studies (28–33), and that 80% of individuals adhered to mask wearing (34–36). 4) Relocation of “high-risk” individuals: moving high-risk individuals (defined as those ≥60 years and/or with co-morbidities) to single hotel rooms, modelled by replacing such individuals with lower-risk individuals. 5) Routine PCR testing of staff only: twice-weekly testing of staff only, assuming 80% compliance. 6) Combination strategy: strategies 1−4 combined. Daily symptom screening (strategy 1) was included in all strategies.
Prediction of impact of infection control strategies
For each intervention strategy we simulated transmission within a shelter of 250 residents and 50 staff (based on an average shelter size) over 30 days starting with one latently infected individual 1000 times (to account for stochastic uncertainty). The time period was chosen to capture the trajectory of an outbreak and differential benefits of strategies. The primary outcome was the probability of averting an outbreak (defined as 3 or more infections originating within the shelter in any 14-day period (37,38)) under each strategy, with secondary outcomes of the proportional reductions in the total numbers of COVID-19 infections and clinical cases, and total numbers of hospitalizations, deaths and PCR tests used. Only individuals who tested positive were removed from the shelter population. The initial population was chosen to have the same composition in terms of proportions in different risk groups (by age and co-morbidity status) as the San Francisco shelter. We estimated the probability of averting an outbreak under each intervention strategy (compared with no interventions) for each calibrated R0 value for a range of different background infection rates estimated from recent incidence of confirmed cases in Seattle, Boston and San Francisco (see Additional file 1 for details). To account for potential upward bias in the estimated R0 range due to fitting to data from shelters with high attack rates, we performed the same simulations for a shelter environment with a low R0 of 1.5. The analyses were conducted in R version 4.0.0 (39) and the data and model code are available at https://github.com/LloydChapman/COVID_homeless_modelling.
Sensitivity analysis
We conducted a multi-way sensitivity analysis to assess the impact of uncertainty in key natural history and intervention parameters − relative infectiousness of subclinical infection and the early infectious stage, sensitivities and specificities of symptom screening and PCR tests, testing and masking compliances, and mask effectiveness − on the results, by simulating each intervention strategy across all combinations of the minimum and maximum values of these parameters over their uncertainty ranges (Table 1). We explored the impact of PCR testing frequency on the probability of averting an outbreak by varying the testing frequency in strategy 2 from daily to monthly.
Results
Model calibration
The model reproduced the numbers of PCR-positive individuals in the cross-sectional surveys in the Seattle and Boston shelters (Additional file 1: Figure S4) and the observed numbers of PCR-positive individuals and symptomatic cases over time for the outbreak in the San Francisco shelter (Additional file 1: Figures S4−S5). The estimated R0 values ranged from 2.9 (95% CI 1.1−6.7) for Seattle shelter B to 6.2 (95% CI 4.0−7.9) for the San Francisco shelter (Additional file 1: Table S7), with corresponding estimated cumulative infection incidences at the end of the testing period of 14% (95% CI 1−41%) and 83% (95% CI 72−92%) (Additional file 1: Table S8). The median estimated number of infections initially introduced was 3 for all shelters (95% CI 1− 5). The estimated date of introduction of infection ranged from 10 days (95% CI 7−14 days) before the first case was identified for Seattle shelter B to 21 days (95% CI 17−26 days) before for San Francisco.
Impact of infection control strategies
Table 2 shows the projected impact of the six infection control strategies considered, for different transmission environments. Daily symptom screening performed poorly across different transmissibilities (probability of averting an outbreak = 0.03 for San Francisco R0 = 6.2, and probability = 0.33 for R0 = 1.5). Relocating individuals at high-risk of clinical symptoms combined with symptom screening performed similarly to symptom screening alone (probability of averting an outbreak = 0.03−0.33 for R0 = 6.2−1.5). Twice-weekly PCR testing of staff provided some additional benefit over daily symptom screening at lower transmissibilities (probability of averting an outbreak = 0.03−0.40 for R0 = 6.2−1.5). Universal masking and twice-weekly PCR testing of all individuals yielded higher probabilities of averting an outbreak of 0.06−0.47 and 0.04−0.52 for R0 = 6.2−1.5. The combination strategy involving daily symptom screening, twice-weekly PCR testing of all individuals, universal masking, and removal of high-risk individuals gave the highest probability of averting an outbreak (0.08−0.68 for R0 = 6.2−1.5), but still prevented a minority of outbreaks in all but the lowest-risk setting.
The probability of averting an outbreak under each intervention strategy decreased with increasing transmission potential (R0) inside the shelter and with increasing infection incidence in the community outside the shelter (Figure 1). Even under the combination strategy, the probability of averting an outbreak in an average-transmission-potential shelter (R0 = 2.9) decreased from 0.58 to 0.07 as the background infection rate increased from 0 to 439 cases per 1 million person-days (the estimated background infection rate in San Francisco between June 27 and July 10, 2020).
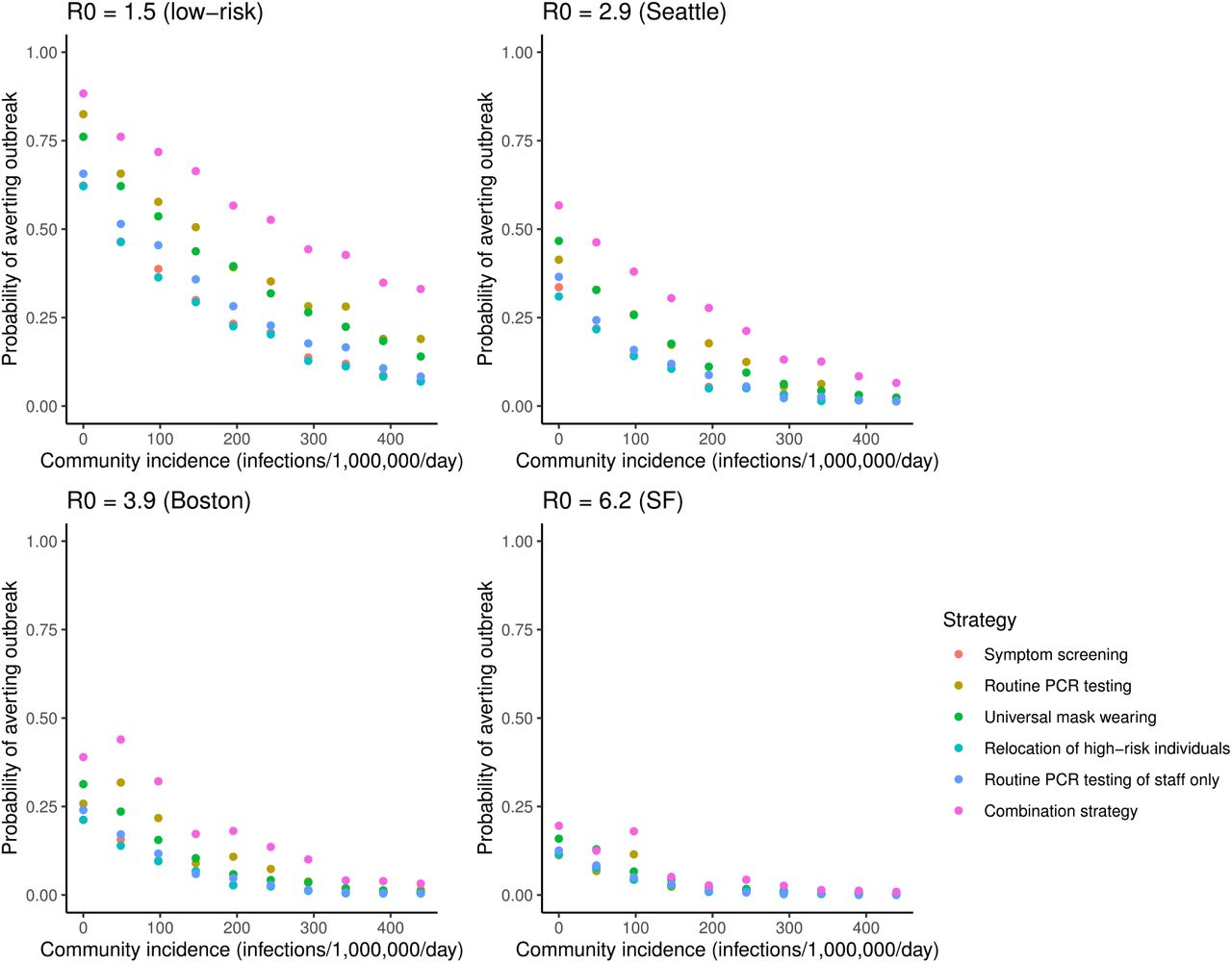
The probability of averting an outbreak (≥3 infections over any 14-day period) in a generalized homeless shelter of 250 residents and 50 staff over 30 days was estimated for different infection incidences in the community using the microsimulation model described in the text. SF = San Francisco.
The relative reduction in infection incidence under the different infection control strategies followed the same pattern as the probability of averting an outbreak (Additional file 1: Table S10 and Figure 2).

Solid lines show mean daily numbers of new infections and shaded areas show minimum and maximum daily numbers over 1000 simulations. Background infection rate in the community outside the shelter of approximately 120 infections/1,000,000 person-days. SF = San Francisco.
PCR test requirements were approximately three times higher (at an average of 6.6 tests per person per month) under twice-weekly PCR testing of all individuals than when only testing individuals identified as symptomatic in daily symptom screening (2.0 tests/person/month), and approximately two times higher than when only testing staff twice-a-week (2.8 tests/person/month) (Additional file 1: Table S11).
Sensitivity analysis
The probability of averting an outbreak was most sensitive to uncertainty in mask effectiveness and relative infectiousness of the early infectious stage, with the mean probability of averting an outbreak across all combinations of the minimum and maximum values of the other parameters varying from 0.36−0.54 for 10−50% mask effectiveness and 0.53−0.36 for early stage relative infectiousness of 1−3 for R0 = 2.9 (Additional file 1: Figure S9). After this, the probability of averting an outbreak was most sensitive to PCR sensitivity and masking and testing compliances, with the mean probability of averting an outbreak varying between 0.39 and 0.51 over the uncertainty ranges of these parameters. Decreasing the frequency of PCR testing from daily to monthly decreased the probability of averting an outbreak for R0 = 1.5, 2.9 and 3.9 from 0.70 to 0.35, 0.27 to 0.12, and 0.23 to 0.08 respectively, but had little impact on the already low probability of averting an outbreak for R0 = 6.2 (Figure 3).

{kind=link}
{kind=link}
{kind=link}
The probability of averting an outbreak (≥3 infections over any 14-day period) over 30 days was estimated for different frequencies of routine PCR testing from daily (1 day between tests) to monthly (30 days between tests). Background infection rate in the local community of approximately 120 infections/1,000,000 person-days. SF = San Francisco.
Discussion
Several outbreaks of COVID-19 with high attack rates have occurred in homeless shelters across the US, and there remains uncertainty over the best infection control strategies to reduce outbreak risk in shelters. In this study, we applied a simulation analysis to identify infection control strategies to prevent future outbreaks. We found that in high-risk shelters that are unable to maximize basic infection control practices that sufficiently reduce the transmissibility of SARS-CoV-2 (e.g. social distancing, reduced living density), no additional infection control strategy is likely to prevent outbreaks. In contrast, in lower-risk shelters with low background community incidence, the implementation of strategies such as symptom screening, routine PCR testing, and masking would help reduce outbreak risk.
We found a wide range of transmissibility of SARS-CoV-2 based on observed outbreaks in homeless shelters, which greatly affects intervention impact. We estimated basic reproduction numbers (R0) of 2.9−6.2 from aggregate PCR test data from outbreaks in five shelters in Seattle, Boston and San Francisco. This range of R0 values is at the high end of estimates reported in the literature (40–43), and likely reflects a high degree of heterogeneity in infectiousness between individuals (42,44–47) and a highly conducive environment for transmission within these shelters due to lack of existing infection control practices and high living density. Our R0 estimates are also likely not entirely representative of general transmission potential in shelters as non-outbreaks and smaller outbreaks may go undetected or unreported, and some shelters have reported only low numbers of infections (4,48). For these R0 values and current background infection rates, we found that the infection control strategies considered are unlikely to prevent outbreaks (probability < 40%), even when combined. Nevertheless, they do reduce incidence of infection and clinical disease and slow the growth of the outbreak (Figure 2).
In a lower transmissibility setting, with R0 = 1.5, e.g. where staff and clients are able to socially distance, the considered intervention strategies are more likely to prevent outbreaks (probability up to nearly 70% under combined interventions, for a moderate background infection rate equivalent to that in Boston in early July of 122/1,000,000/day).
A key remaining issue is identifying the characteristics that distinguish low-risk shelters that can be safely operated with implementation of infection control strategies. Data is limited, but available evidence suggests that social distancing and reductions in super-spreading are likely to be key factors (42,44,49–51). Strategies that may achieve these goals include reducing living density, spacing bedding, reducing communal activities, and adopting staffing models that limit social contacts.
The fact that intervention impact and the probability of averting an outbreak decrease significantly with increasing background infection rate in the community (Figure 1) suggests a need for alternative housing arrangements for people experiencing homelessness in locations in which community incidence is moderate to high − 100−500 infections/1,000,000/day, equivalent to 25−125 confirmed cases/1,000,000/day (i.e. current San Francisco incidence) assuming four-fold underreporting (see Additional file 1). In lower background incidence settings, combined daily symptom-based screening, twice-weekly PCR testing, universal masking and relocation of high-risk individuals to non-congregate settings would reduce outbreak risk, and limit incidence of infection and severe disease if outbreaks do occur.
Each infection control strategy is limited in some aspect (22,52–56). Symptom-based screening has very low sensitivity to detect infections early in the clinical course (when people are most infectious), and poor specificity (12–14,57). The impact of routine PCR testing is limited by imperfect PCR sensitivity (∼75%), especially early in the infection course (18), as well as need for frequent testing and missing onset of infectiousness between testing periods. Other analyses support our finding that testing less than once or twice weekly leaves a high risk of outbreaks (e.g. testing once every two weeks gives a 30% lower probability of averting an outbreak than twice-weekly testing, Figure 3) (15–17). However, once- or twice-weekly testing may be financially and logistically infeasible. Similarly, relocation of high-risk persons to independent housing is resource intensive. Frequent testing and universal masking also suffer issues with adherence, which constrains their effectiveness.
This study has a number of limitations. Due to limited data availability, we only calibrated the model to a small number of shelter outbreaks, the R0 estimates for which are likely to be higher than for the average shelter due to larger outbreaks being more likely to be reported. The cross-sectional aggregate nature of the majority of the data also led to wide uncertainty intervals around the fitted parameters, without independent identifiability between them (Additional file 1: Figure S10). Our estimate of the impact of masking is highly sensitive to the assumed effectiveness of masking, which has mixed evidence (28,29,31). Many uncertainties in the biology of SARS-CoV-2 transmission remain, particularly regarding differential infectiousness over time and by severity of illness, and the relationship of PCR positivity and infectiousness (22,58,59). Our assumption of equal infectiousness for different individuals means that our model is unlikely to fully reproduce super-spreading events (42,44). We made several simplifying assumptions in modelling transmission within the shelter and from the surrounding community, namely: homogenous mixing within the shelter population, no entry of new people, a stable background infection rate over time and full immunity upon recovery from infection given the short duration of the simulation. We assumed homogeneous mixing due to a lack of contact data for the shelter outbreaks, which meant that we were not able to consider cohorting and contact tracing as interventions.
This study defines conditions that would support safely operating homeless shelters with lower risk of COVID-19 outbreaks and estimates the impact of various interventions on outbreak risk. Our findings demonstrate the need for combined interventions (symptom-based screening, PCR testing, and masking) and regular testing to protect persons experiencing homelessness from COVID-19, while highlighting the limitations of these interventions in preventing outbreaks.
Data Availability
All data and code used for the analysis are available at: https://github.com/LloydChapman/COVID_homeless_modelling
Ethics approval and consent to participate
This study was considered exempt non-human subject research based on use of de-identified secondary data by the University of California, San Francisco Institutional Review Board.
Consent for publication
Not applicable.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available online at https://github.com/LloydChapman/COVID_homeless_modelling.
Competing interests
The authors declare that they have no competing interests. NCL has received funding from the World Health Organization for unrelated work.
Funding
This work was supported by the University of California, San Francisco (UCSF) and the UCSF Benioff Homelessness and Housing Initiative. The funders had no role in the study design, data collection and analysis, preparation of the manuscript, or the decision to submit the manuscript for publication.
Authors’ contributions
NCL conceived the study. LACC and NCL designed and conducted the analysis and drafted the manuscript. SNC, AS, CC, TN, EI acquired and curated the data from the San Francisco shelter outbreak. NCL and MK acquired funding. All authors contributed to, read, and approved the final manuscript. LACC and NCL had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Supporting information
Additional file 1 (pdf): Supplementary methods and results: Details of the model and model calibration. Table S1: Definition of states in the transmission model. Table S2: Risk of clinical symptoms and hospitalization by age group and co-morbidity status. Table S3: Numbers of PCR-positive individuals by day of test result and daily new symptom onsets in San Francisco shelter March 28–April 10, 2020. Table S4: Numbers of residents and staff PCR tested and PCR positive at three shelters in Seattle during two testing events March 30–April 1, 2020 and April 7–8, 2020. Table S5: Input parameters for microsimulation of COVID-19 transmission in homeless shelters. Table S6: Different intervention strategies tested. Table S7: Estimated epidemiologic parameters based on observed outbreak data from homeless shelters in Seattle, Boston and San Francisco. Table S8: Estimated cumulative infection incidence at the end of the PCR testing period in homeless shelters in Seattle, Boston and San Francisco. Table S9: Probability of averting an outbreak over a 30-day period in a generalized homeless shelter with simulated infection control strategies for different background infection rates in the community outside the shelter. Table S10: Reductions in the total number of infections and symptomatic cases over a 30-day period in a generalized homeless shelter with simulated infection control strategies for different background infection rates in the community outside the shelter. Table S11: Numbers of PCR tests used under each infection control strategy. Figure S1: Structure of stochastic individual-level susceptible-exposed-infectious-recovered (𝒮-ℰ-𝒥-ℛ) model of COVID-19 transmission in homeless shelter. Figure S2: Daily numbers of residents by risk group present in the San Francisco shelter March 29–April 10, 2020. Figure S3: Distribution of duration of detectable viral load from start of late infectious stage. Figure S4: Calibration of microsimulation to observed PCR testing data from outbreaks in homeless shelters in Seattle, Boston and San Francisco. Figure S5: Calibration of microsimulation to additional data from San Francisco shelter outbreak. Figure S6: Outbreak size distributions 30 days after introduction of infection in a generalized homeless shelter under different infection control strategies for R0 = 1.5 (low-risk setting). Figure S7: Outbreak size distributions 30 days after introduction of infection in a generalized homeless shelter under different infection control strategies for R0 = 2.9 (Seattle). Figure S8: Outbreak size distributions 30 days after introduction of infection in a generalized homeless shelter under different infection control strategies for R0 = 6.2 (San Francisco). Figure S9: Spider diagrams showing the sensitivity of the estimated probability of averting an outbreak to variation in key natural history and intervention parameters for different R0 values. Figure S10: Posterior distributions and pairwise correlation plots for calibrated model parameters – R0, E0 and T – for (A)-(C) Seattle shelters A–C, (D) Boston shelter and (E) San Francisco shelter
Acknowledgements
We sincerely appreciate the hard work and public health efforts of all those involved in the collection of the data used in this article. LACC would like to thank Renata Retkute, Amanda Minter, Simon Spencer and TJ McKinley for helpful discussions regarding Approximate Bayesian Computation.
Footnotes
Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
- CI
- credible interval
- COVID-19
- Coronavirus disease 2019
- PCR
- polymerase chain reaction
- SARS-CoV-2
- Severe acute respiratory syndrome coronavirus 2
- UI
- uncertainty interval
- US
- United States
References



