
Abstract
Objective This research aimed to systematically review and summarize the influence of Renin-Angiotensin-Aldosterone System (RAAS) inhibitors on the outcome of COVID_19 patients with hypertension.
Methods Electronic databases; PubMed/Medline, CINAHL, the Cochrane Central Register of Controlled Trials, clinical trial.gov, and Google Scholar were searched from 2019 to June 1, 2020. Additionally, the references of identified articles were also searched.
Results A total of 9 articles comprising 3,823 patients were incorporated; 1416 patients on RAAS inhibitors and 3469 on non-RAAS inhibitors. The study demonstrated that the taking of RAAS inhibitors in COVID_19 patients with hypertension significantly reduced mortality where patients on RAAS inhibitors had a 27% decrease of mortality (RR = 0.73 [95% CI: 0.63- 0.85, p< 0.0001, I2 = 0%, random-effects model]) compared to those not taking ACEI/ARB. No significant association were observed in disease severity (RR = 0.92 (95% CI: 0.74- 1.14) and hospitalization (WMD = –2.33[95% CI: –5.60, 0.75]), random-effects model.
Conclusion This study supports RAAS inhibitors’ safe use among COVID_19 patients with hypertension.
Background
Corona viral diseases 2019 (COVID_19) is a pandemic disease originated from Wuhan city of, China from December 20191. The pandemic has continued to debilitate global health and the economy. As of June 7, 2020; 7,005,822 cases of COVID_19 were reported, including 402,678 deaths worldwide2. Severe COVID_19 illnesses have consistently been observed in patients with Comorbid illnesses such as cardiovascular and diabetes mellitus3. According to the report of the Chinese CDC as of February 11, 2020, 10.5% of deaths occurred in COVID_19 patients with cardiovascular diseases and, 6% of them were patients with hypertension3.
Most patients with cardiovascular disease use RAAS inhibitors; commonly angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB)4. They are a drug of choice for heart failure, hypertension, chronic kidney disease and, myocardial infraction5, 6. Besides inhibition of the formation of angiotensin II; RAAS inhibitors increase the expression of angiotensin-converting enzyme 2 (ACE2); a membrane-bound aminopeptidase that is expressed abundantly in the lungs and the heart7. ACE2 plays an important role in the breakdown of angiotensin II (a potent vasoconstrictor) to angiotensin (1–7) (a vasodilator)8 which helpful in cardiovascular patients.
Researches reported that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) attacks the humans cells through ACE29, 10, and reduces ACE2 expression, resulting imbalance of ACE/Ang II/AT1R axis and ACE2/Ang (1–7)/Mas receptor11, 12. Therefore; there are concerns about the use of RAAS inhibitors as a result of an increase in expression of ACE2; a target molecule for SARS CoV-213–15. This led to the hypothesis that the use of RAAS inhibitors might be harmful in patient with COVID_19 especially in patients with comorbidity like hypertension. There are retrospective studies conducted to test this hypothesis and one meta-analysis (preprint)summarized the studies in all patients taking RAAS inhibitors16. The meta-analysis included 1842 COVID_19 patients and exhibited a significant 43 % decrease in mortality on the side of patients taking ACEI/ARB16. After the meta-analysis several studies were conducted which requires updating the evidence and also there is a need for evidence on hypertensive patients. This study aimed to systematically synthesis the evidence on the effect of RAAS inhibitors on the outcome of COVID_19 patients with hypertension.
Methods
Study design
This is a systematic review and meta-analysis conducted using electronic database searches. The review conducted according to the preferred reporting items for Systematic Review and Meta-Analysis Protocol (PRISMA)17. The protocol was registered in the (Prospero) International Prospective Register of a systematic review with registration number CDR42020186477.
Search strategy
The databases such as PubMed, the Cochrane Central Register of controlled trials, clinical http://trial.gov, CINAHIL, and Google scholar were searched from 2019 to June 1, 2020. Additionally, the references of identified articles were also searched. No language limitation was employed. Flow diagram was used to summarize the number of studies identified, screened, excluded, and finally included in the study. Search terms for PubMed were attached under the supplementary document (Appendix 1).
Study selection
Two reviewers (TB and TS) independently carried out searching for literature and identified relevant studies and sequentially screened their titles and abstracts for eligibility. The full texts of eligible studies were retrieved. Differences in the inclusion of articles were fixed on discussion with the third author (SD). A screening guide was used to ensure that all review authors applied the selection criteria.
Inclusion criteria
Randomized controlled trials (RCTs) including cluster RCTs, observational studies, and prospective, retrospective comparative cohort studies and case-control studies were considered to be included in the systematic review and meta-analysis. The review considered all patients who were taking ACEI or ARBs alone or in combination for hypertension with COVID-19 patients.
Exclusion criteria
In vitro studies, studies not related to ARB or ACEI for COVID-19 patients with hypertension, studies without extractable data, outcome (death), or severity or hospitalization not clearly reported were excluded from the review.
Methodological quality assessment
Selected papers were evaluated by two reviewers (TB & TS) for methodological validity before inclusion in the review with the Newcastle-Ottawa quality assessment score (NOS) method. Any differences that arose from the reviewers were fixed through discussion, with a third reviewer (SD).
Data extraction
Two reviewers (TB and TS) extracted data from the studies using a pre-designed format. Data extracted include first author, the region of study, included population, study design, number of study participants, comparator group, patient status, severity, age (mean, median), gender, interventions, and patients outcomes (number of cases).
Data analysis and statistical methods
Data analysis was performed by RevMan 5.4 (Copenhagen: the Cochrane Collaboration, 2020) and Stata version 13 (StataCorp, 2013). Risk ratios were used for comparison and reported as 95% confidence interval. P-value ≤ 0.05 was considered statistically significant. The Q-statistic test was used to assess the heterogeneity of the included study and I2 statistic was used to indicate the percentage of variation in the studies as a result of heterogeneity instead of chance.
Results
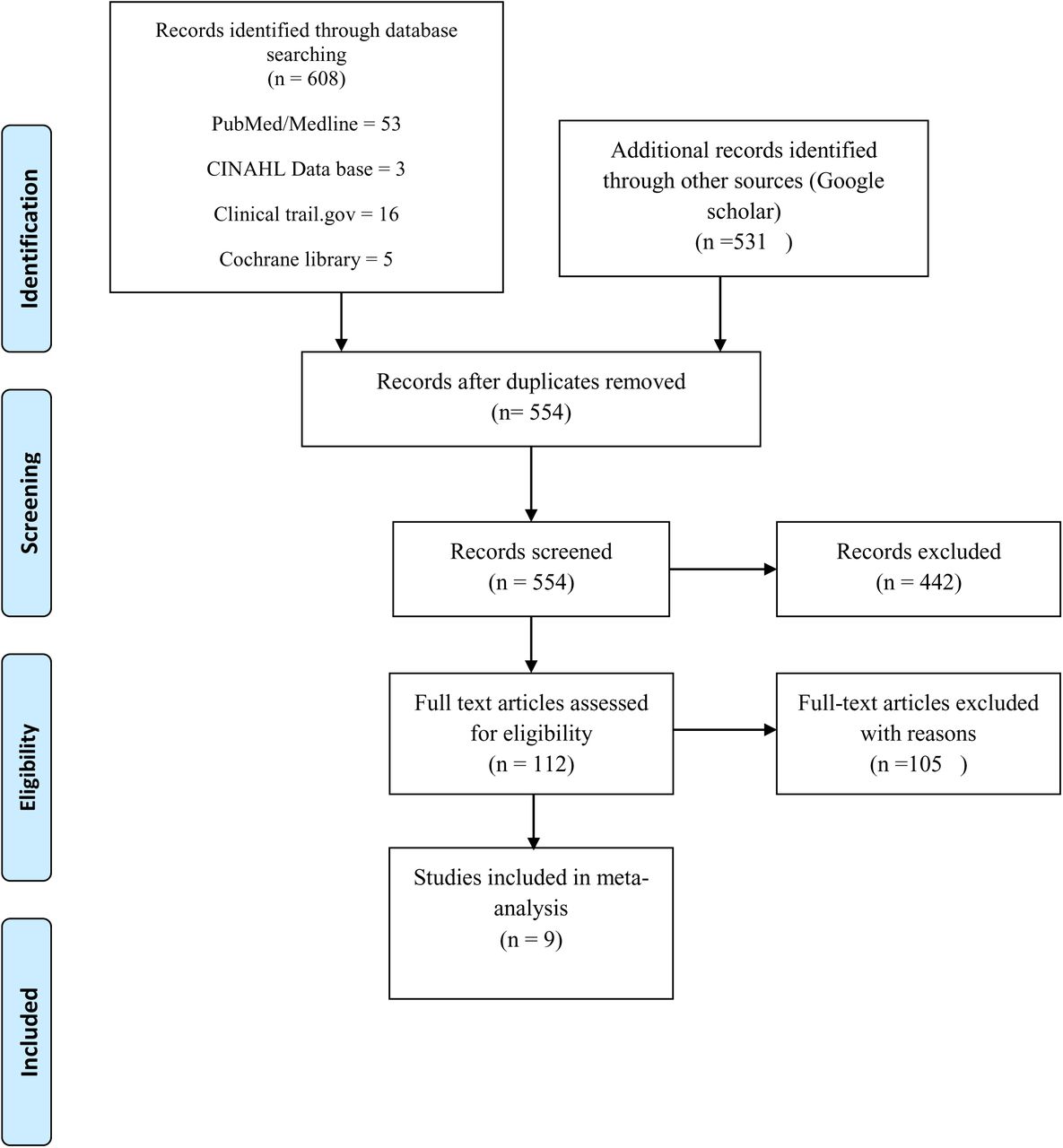
A total of 608 articles were identified through searching of electronic databases, out of this 554 remained after removing duplications. After screening in title and abstract 112 articles remained; of which 105 articles (review articles and letters to editors) were excluded. Finally, 9 articles were included for meta-analysis18–26 (Fig 1). A total number of 3,823 patients were included; 1416 patients on RAAS inhibitors and 3469 on non-RAAS inhibitors (Fig 2). Newcastle-Ottawa Scale methodological quality assessment gave the quality of the included studies in good arrangement (Appendix 2).
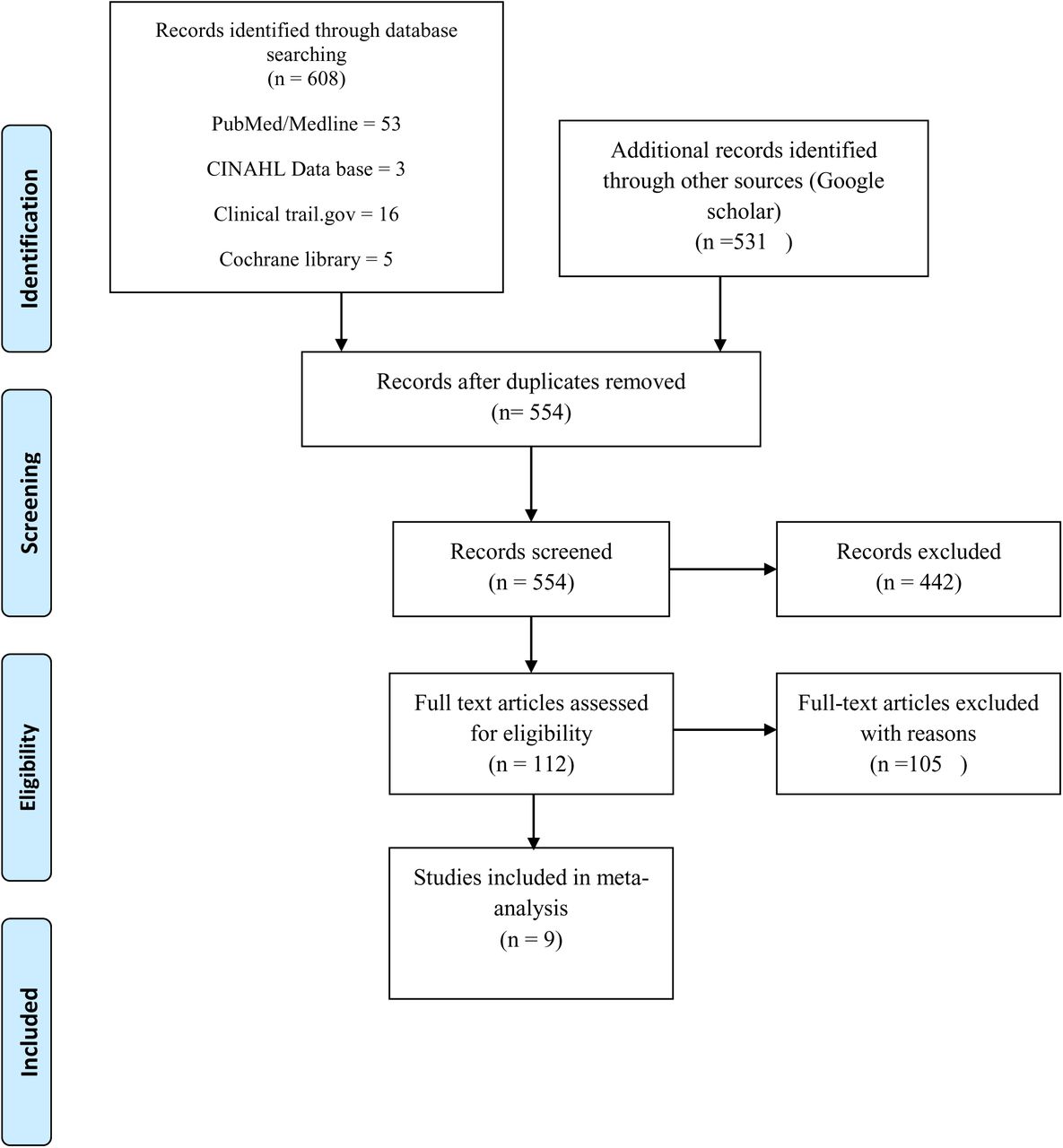
PRISMA flow diagram showing, screened, excluded and included studies
All included studies were retrospective, and six were conducted in China, one in USA and one in UK, (table 1).

Forest plot for severity of patients taking RAAS inhibitors compared to those not taking RAAS inhibitors.
Effect of RAASI on disease severity
Nine studies reported the severity data of the hypertensive COVID-19 patients. No significant association was observed with RAAS inhibitors on severity; RR = 0.92 (95% CI: 0.74–1.14), random effect model. Significant heterogeneity was observed among the studies (I2 = = 64%, P = 0.005)Fig. 2.
Effect of RAAS inhibitors on mortality of patients with COVID_19 and hypertension
Seven studies reported the mortality data of the hypertensive COVID_19 patients. No heterogeneity was observed among the 7 studies (I2 = 0%, P = 0.59). The pooled mortality was RR = 0.73 (95% CI: 0.63- 0.85), fixed effect model Fig. 3.

Forest plot for mortality of patients taking RAAS inhibitors compared to not taking RAAS inhibitors
The use of RAAS inhibitor did not have association with long term hospitalization as compared with non RAAS inhibitor users (weighed mean difference –2.33[95% CI: –5.60, 0.75], fixed effect model. No heterogeneity was observed (I2 = 0%, P = 0.65), Fig 4.

Effect of RAAS inhibitor on the time of hospitalization
Assessment of bias
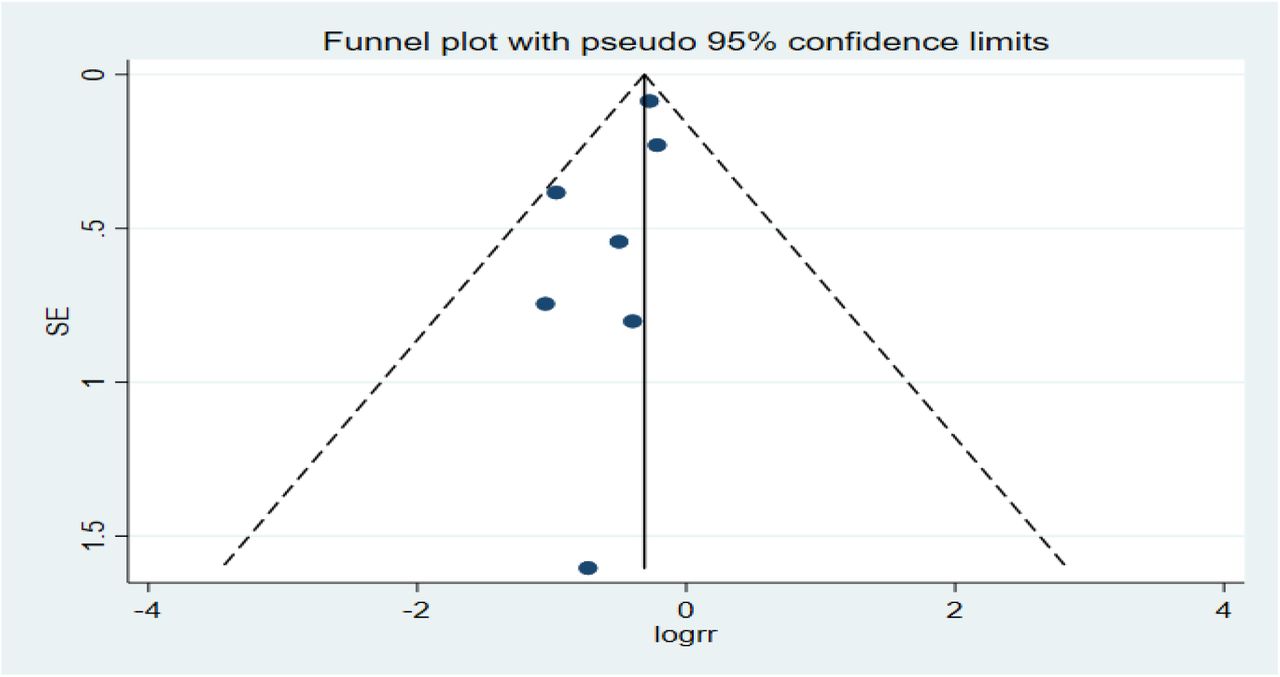
The funnel plot was used to assess the publication bias. Funnel plot indicates the existence of small study effects. We performed the regression–based on Egger’s test. The funnel plot was symmetrical in shape for severity and mortality (Fig 5 and 6), indicating no publication bias. Regression-based Egger’s test indicates that there were no small-study effects on mortality (P = 0.122) and severe events (p = 0.686).

Funnel plot for the severity of diseases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot for mortality
Discussion
Concern over the safety of RAAS inhibitors use in patients contracted COVID_19 originated since SARS-CoV-2 uses ACE2 receptor to enter the target human cell. Animal studies also showed an increase in RAAS inhibitor expression of ACE2 which could speed up the spread of the virus in human cells, predispose for hospitalization, increase and, mortality. This was further strengthened by the report that patients with hypertension taking ACEI/ARB have increased risk of developing severe pneumonia (P = 0.064)22. Dooley et al. also reported that RAAS inhibitors increased the risk of symptomatic infection with COVID_19 approximately by two-fold in community populations27. However, other studies reported that the use of ACEI/ARB did not show association with the outcome of COVID-19 patients28–31.
This study, however, was in contrast to the original hypothesis demonstrating the safe usage of RAAS inhibitors in hypertensive COVID_19 patients; in this, it was associated with a significant reduction in mortality. The hypertensive patients with COVID_19 who were on ACE/ARB had a 27% reduction in risk of mortality compared to that not on ACEI/ARB. This finding is helpful and should be considered in clinical decision making. Two large sample size studies,18 and21, reported a reduction in mortality with patients on ARBs/ACEIs compared to those on non-ARBs/ACEIs medications. A study compared the use of other antihypertensive drugs with ACEI/ARB revealed that ACEI/ARB significantly reduced mortality in COVID_19 patients with hypertension23. RAAS inhibitors thought to up-regulate the level of ACE2 which may protect against organ damage by inhibiting the production of angiotensin II32. Moreover, the study showed that patients with COVID_19 appeared to exhibit RAAS activation, increased viral load levels, and lung injury33. However, all five small sample studies did not show any association with mortality20–24. Emerging data suggested that patients with hypertension and diagnosed with COVID_19 are at an increased risk of death34. These patients have often prescribed RAAS inhibitors, including ACE inhibitors35 and ARBs36. The finding of this study indicated the beneficial effect of RAAS inhibitors use over not using them and correlated well with the recommendation of the International Society of Hypertension37.
This study showed no significant association in both severities of the disease and hospitalization. Previously reported studies revealed the direct anti-inflammatory effect of RAAS inhibitors which could help in the prevention of cardiovascular complications38. RAAS inhibitors reduce pro-inflammatory cytokines, chemokine’s; reduce pro-inflammatory effect leukocyte, and endothelial cells39. This could justify the current findings and lower number of critical patients in hypertension patients with COVID-19 on RAAS inhibitors arm. However, fewer study availability and retrospective nature of the included studies warrants further randomized controlled studies and observational studies.
Conclusion
This study supports the safe use of ACEI/ARB among hypertensive patients contracted COVID_19 and in line with the recommendation of the International Society of Hypertension.
Data Availability
N/A
Ethical approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interest
Funding
No funding received for this study
Authors’ contribution
TBB and TS designed the study, searched literature, analyzed data and drafted manuscript. SD interpreted and reviewed the result. All authors participated, reviewed and approved the final manuscript.
Acknowledgment
Not applicable
Appendix 1: Search terms used
(“ace inhibitor*” OR “angiotensin converting enzyme inhibitor*” OR arb*, “angiotensin receptor blocker*” OR captopril OR capoten OR benazepril OR Lotensin OR enalapril OR vasotec OR epaned OR lexxel OR fosinopril OR monopril OR lisinopril OR prinivil OR zestril OR qbrelis OR moexipril OR univasc OR perindopril OR aceon OR quinapril OR accupril OR ramipril OR altace OR trandolapril OR mavik OR teveten OR benicar OR olmesartan OR diovan OR valsartan OR atacand OR candesartan OR cozaar OR losartan OR micardis OR avapro OR edarbi OR irbesartan OR “azilsartan medoxomil” OR prexxartan OR valsartan) AND (“sarscoronavirus” OR “sars-cov-2” OR “severe acute respiratory syndrome” OR coronavir* OR coronovirus* OR “corona virus” OR “corono virus” OR “corono virus” OR “virus corona” OR “virus corono” OR “covid-19” OR “covid19”* OR “covid 19” OR “2019-nCoV” OR (wuhan* AND (virus OR viruses OR viral)) OR (covid* AND (virus OR viruses OR viral)) OR “sars-cov” OR “mers-cov” OR “mers cov” OR “middle east respiratory syndrome”).
Appendix 2: Newcastle–Ottawa Scale (NOS) methodological quality assessment
Interpretation
Good quality: 3 or 4 stars from selection; 1or 2 stars from comparability and 2 or 3 stars from outcome
Fair quality: 2 stars in selection; 1 or 2 stars in comparability and 2 or 3 stars in outcome
Poor quality: 0 or 1star from selection OR 1 or 2 stars in comparability OR 0 or 1 star from outcome
Footnotes
Email address: TBB tamiratbekele12{at}gmail.com, TS tamepfsa{at}gmail.com; SD dserawit{at}std.must.ac.ug
List of abbreviations
- COVID_19
- Corona viral diseases 2019
- SARS-CoV-2
- severe acute respiratory syndrome coronavirus 2
- CDC
- Center of Disease Control
- RAAS
- renin-angiotensin-aldosterone system
- ACEI
- Angiotensin-converting enzyme inhibitors
- ARB
- Angiotensin receptor blocker
- ACE2
- angiotensin-converting enzyme 2
- Ang II
- Angiotensin II
- PRISMA-P
- Systematic Review and Meta-Analysis Protocol
- RCTs
- randomized controlled trials
- CCB
- Calcium channel blocker.
References



