
ABSTRACT
BACKGROUND Although the infection rate of COVID-19 is very high, all the patients getting infected don’t always die or go through brutal states. This indicates there may be some factors that possibly boost the severity of COVID-19.
OBJECTIVE We intend to identify some probable risk factors that are responsible for the severity of COVID-19 using a meta-analysis.
METHODS The literature exploration lasted up to 18 April 2020 and through PubMed, Google Scholar, EMBASE, and Cochrane Library we have identified 10 pertinent publications. To paraphrase the outcomes of autonomous researches, we have performed a random-effect meta-analysis.
RESULTS A total of 2272 patients’ information was extracted from the selected literature. We have found sex (male) (Risk ratio [RR] =1.29 [1.07; 1.54]), hypertension (RR=1.79 [1.57; 2.04]), diabetes (RR=1.57 [1.25; 1.98]), fatigue or myalgia (RR=1.17 [1.02; 1.35]), and smoking history (RR=1.71 [1.25; 2.35]) are potential risk factors for the severity of COVID-19. We found fever (RR=1.21 [0.66; 2.22]), cough (1.13 [0.98; 1.30]), and diarrhea (RR=1.14 [0.93; 1.40]) as insignificant risk factors for COVID-19 severity.
CONCLUSION The findings of this research may be beneficial to identify patients with higher risks to provide additional medical attention from the very beginning of the treatment.
INTRODUCTION
The coronavirus disease 2019 (COVID-19) originated from Wuhan (Hubei state, China), carrying similar DNA structure to SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome) has spread throughout the world and creating massive panic to the human life1,2. The disease has the worst feature to transmit from person to person3, considering this feature and its lofty infection rate on January 30, 2020, the World Health Organization (WHO) declared COVID-19 as a global emergency.
To date, it has infected more than 3 million people and over 2 lakh have died. The outbreak has hit the USA, Italy, and Spain very badly. This three-country together holds over 1.3 million total identified cases and over 50% of the total death because of COVID-194. As no proven treatment/medicine or vaccine is available to date5 the harm of COVID-19 has already overtaken SARS and MARS6.
Although the infection rate is very high, all the patients getting infected by this disease don’t always die. The global recovery rate is about 28.6% and the death rate is about 7% until April 28, 20204. This information suggests that there may be some factors that influence the risk of death or critical medical states of the patients. That’s why it is important to identify and estimate such risk factors to predict the severe complication of the patients for avoiding or to minimize the severity7.
Researchers are trying to identify risk factors that deteriorate the health state of the COVID-19 patients mostly by using meta-analysis and systematic review. Some earlier investigations reported males are more likely to die or to go through the critical states of COVID-198,9. There is an ongoing debate on whether smoking is a risk factor for COVID-19 severity. Although some regard it as a risk factor9,27, others found no significant alliance between smoking and the severity of COVID-198,10. Other clinical traits termed as risk factors in the publications are hypertension11,12, diabetes12,13, and fever8.
In this study, we endeavor to identify some demographic and clinical characteristics which can be appraised as risk factors for the severity of COVID-19 by summarizing findings of the published literature.
METHODS
LITERATURE SEARCH
The literature search lasted from April 2, 2020, to April 18, 2020. Both of the authors searched through PubMed, Google Scholar, EMBASE, and Cochrane Library using keywords: “COVID-19”, “Novel Coronavirus”, “COVID-19 characteristics”, “COVID-19 patient”, and “China coronavirus”. We initially identified all the studies conformed to the keywords without any further investigations.
INCLUSION CRITERIA
Based on the following criteria, we have included literature in the current study: a) bivariate data available for the severity (death/ICU (Intensive Care Unit)/severe state/others) of COVID-19 patients, b) multiple factors available for the severity of the disease, c) full-text access to the article, d) information presented in English language, e) peer-reviewed accepted/published articles, and f) literature published in and after December 2019 (after the first patient identified). We illustrate the systematic selection procedure of literature in Figure 1.

Flow chart showing the study selection procedure
OUTCOMES AND COVARIATES
The authors extracted the number of patients that have undergone the severity of COVID-19 and are stable/recovered under various factors like sex, smoking history, fatigue or myalgia, cough, fever, diarrhea, hypertension, and diabetes. The term severity in this study represents death/ICU/severe state or any other critical medical state. We also extracted the authors’ names, publication year, study design, sample size, country, and other related information from the finally selected studies.
STATISTICAL ANALYSIS
Considering the primary goal of the study we performed random effect meta-analysis where the effect sizes were computed from the raw information dragged from individual studies. We considered the effect size for the study to be a Risk Ratio [RR] and reported with a 95% confidence interval. I2 statistic reported in the forest plot reflects relative between studies heterogeneity and P value (two tail with level 0.05) determines the significance of the heterogeneity test. Microsoft Excel 2013 was used to create metadata, get their univariate characteristics, and export to other software for further analysis. Random effect meta-analysis and relevant forest plots were generated using statistical software R version 3.5.1.
RESULTS
We have extracted 2272 patients’ information from 10 autonomous studies14–23 and incorporated them into this research. The highest sample size for the isolated study was 1099, and 34 was the smallest sample size, other study characteristics are summarized in Table 1.
Characteristics of the selected literatures
Table 2 demonstrates that the bulk of the COVID-19 patients included in the study through a methodical scheme are male (60%). The clinical characteristics of the patients comprise diabetes (11.2%), hypertension (21.3%), fever (90.2%), cough (65%), fatigue or myalgia (41.0%), and diarrhea (9.2%). Only 11.3% of the patients smoke cigarettes (current or past smoker).
Baseline characteristics of COVID-19 patients for different studies
Forest plot in (Figure 2) illustrates that only six studies were entailed for the meta-analysis for characteristic smoking history where all ten studies availed information about the sex of the patients. From the random-effect meta-analysis, we see that patients with smoking history have a higher risk to experience a severe state of COVID-19 (RR =1.71; 95% CI, 1.25 to 2.35) or 71% higher risk pertained to a non-smoker patient. The pooled risk ratio for the male suggests higher risk compared to female patients (RR=1.29; 95% CI, 1.07 to 1.54). In both cases between-study heterogeneity is low and the test of heterogeneity is insignificant (I2=38%, P=0.15; and I2=33%, P=0.15, respectively).

Forest plot for factors smoking history and sex (male) illustrating the distribution of the risk ratio of COVID-19 severity
Figure 3 displays individual and pooled risk ratios for patients with diabetes and hypertension. Although six isolated studies data implies that diabetes is an insignificant risk factor but the overall effect is significant and indicates a higher risk to undergo brutal state for a patient with diabetes (RR =1.57; 95% CI, 1.25 to 1.98). The heterogeneity is moderate (I2=54%) and the test for heterogeneity is significant (χ2=19.59, P=0.02). Also, patients with hypertension have a higher risk (RR=1.79; 95% CI, 1.57 to 2.04) compared to patient those are not suffering from hypertension with insignificant heterogeneity, I2=0% (P=0.50).

Forest plot for factors diabetes and hypertension illustrating the distribution of the risk ratio of COVID-19 severity
Respectively eight and nine studies were involved in the analysis for factors diarrhea and fatigue or myalgia of patients (Figure 4). In both cases the heterogeneity is very low and is insignificant (I2=8%, P=0.37) and (I2=0%, P=0.86), respectively). The pooled random effect infers diarrhea have an insignificant impact on the severity of COVID-19 (RR=1.14; 95% CI, 0.93 to 1.40). But the overall RR=1.17 (95% CI, 1.02 to 1.35) suggests that patients with fatigue or myalgia have a 17% higher risk to go through a severe state of COVID-19.
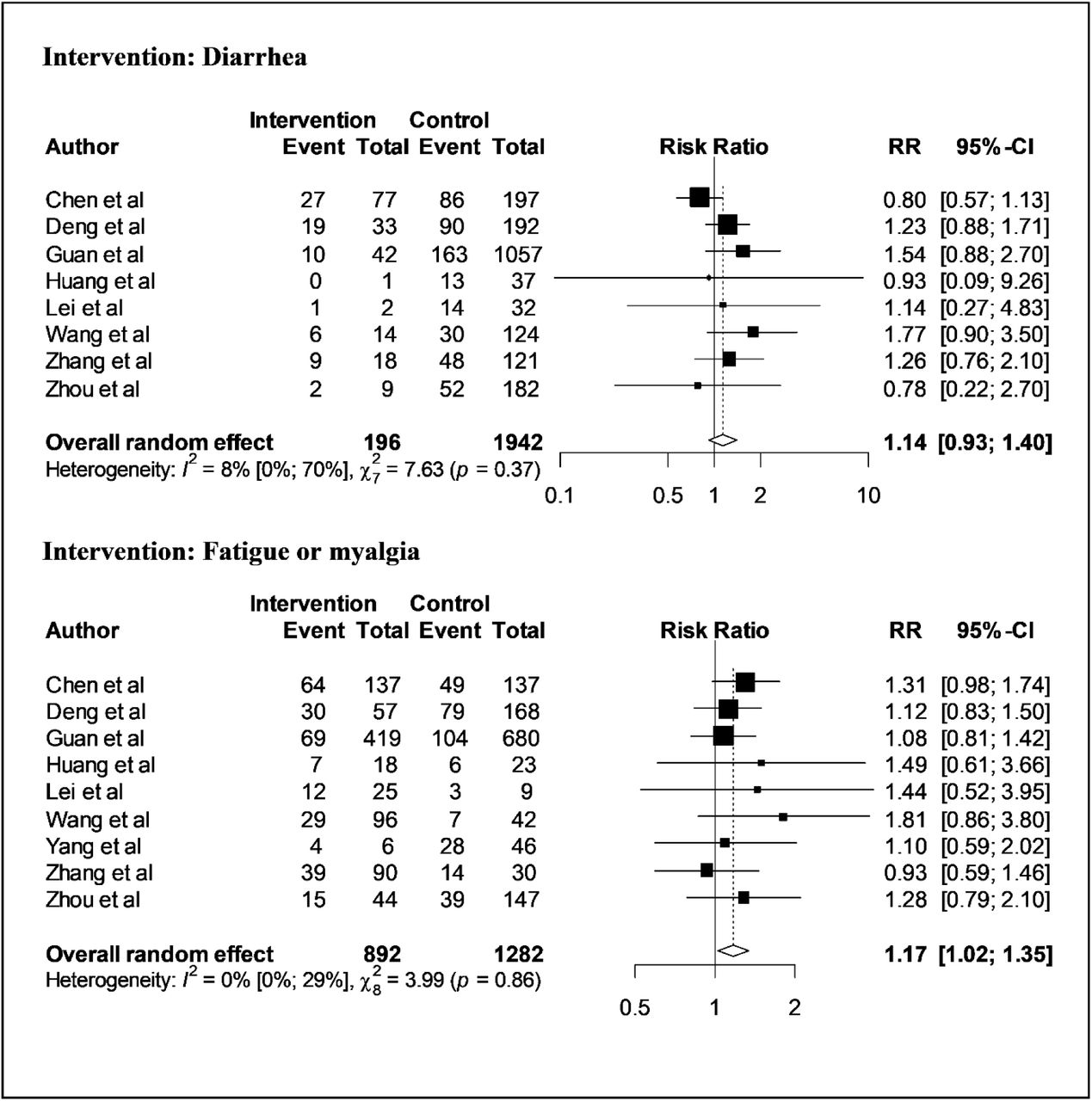
Forest plot for factors diarrhea and fatigue or myalgia illustrating the distribution of the risk ratio of COVID-19 severity
From (Figure 5), we glimpse that cough and fever have no considerable relation with the severity of COVID-19. The pooled effect reflects patient with cough symptom has RR=1.13 (95% CI, 0.98 to 1.30) and patient with fever has RR=1.21 (95% CI, 0.66 to 2.22). Although for cough symptom the between-study heterogeneity is nil and insignificant (I2=0%, P=0.48), it is very big and also significant for fever (I2=85%, P<0.01).

Forest plot for factors cough and fever illustrating the distribution of the risk ratio of COVID-19 severity
DISCUSSION
This study through an organized way incorporated 10 publications and performed a random-effect meta-analysis to identify some risk factors that are probably accountable for the severity of COVID-19. Although none of the articles incorporated in the current research reports any effect size, we computed the effect size (risk ratio) from the published data. The pooled effect size with confidence interval deemed to avouch a factor as a significant risk factor.
We found male patients have a reasonably higher risk to undergo the severity of COVID-19 compared to female patients echoing with some previous studies8,9. An explanation of this can be, the male has weaker immunity because of genetic and hormonal factors and has shown higher mortality in several infectious diseases24,25.
Although some aforementioned studies8,10 found smoking as an insignificant factor to worsen the state of COVID-19 patients, we have found smoking as a significant factor. Smoking is associated with lower or impoverished immunity of smokers26, which can explain why smokers might have elevated risks. Some previous studies9,27 supports our finding, they documented smoking as a significant risk factor, and smokers have a higher risk to undergo a severe state of COVID-19. In a previous study28, smoking was also reported as a risk factor for the critical illness of MERS (Middle East Respiratory Syndrome) too.
We incorporated some clinical traits of the patients like cough, fever, fatigue or myalgia, diarrhea, diabetes, and hypertension in this study. Among those, we have found fatigue or myalgia, hypertension, and diabetes are significant risk factors that might lead to a critical state of COVID-19 patients. Some previous studies8,12,13 also reported both diabetes and hypertension are significant risk factors of COVID-19 progression. These two comorbidities negatively affected MERS-CoV patients’ too29.
From the random-effect meta-analysis, we conclude fever, cough, and diarrhea are insignificant risk factors for the severity of COVID-19. But a previous meta-analysis8 published fever as a significant risk factor for the severity of COVID-19.
CONCLUSIONS
In conclusion, we consider sex (male), smoking history, diabetes, hypertension, and fatigue or myalgia are significant risk factors for the severity of COVID-19. It may require additional medical attention for patients with higher risk from the very beginning of the treatment. We also hope the findings of this study may assist experts in vaccine development programs.
Data Availability
The studies are available online and full-text accessible.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
None declared.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}