Reorganization Tips from a Sarcoma Unit at Time of the COVID-19 Pandemic in Italy: Early Experience from a Regional Referral Oncologic Center


Abstract
:1. Introduction
2. Materials and Methods
2.1. Local Setting
2.2. General Rules
2.3. Sarcoma Unit Approach
2.3.1. New Cases
2.3.2. Already-Known Patients
2.3.3. Urgent Orthopedic Consultation from Other Hospitals
2.3.4. Inter-hospital Inpatient Transfer
2.3.5. Institute Entrance Check Point Screening
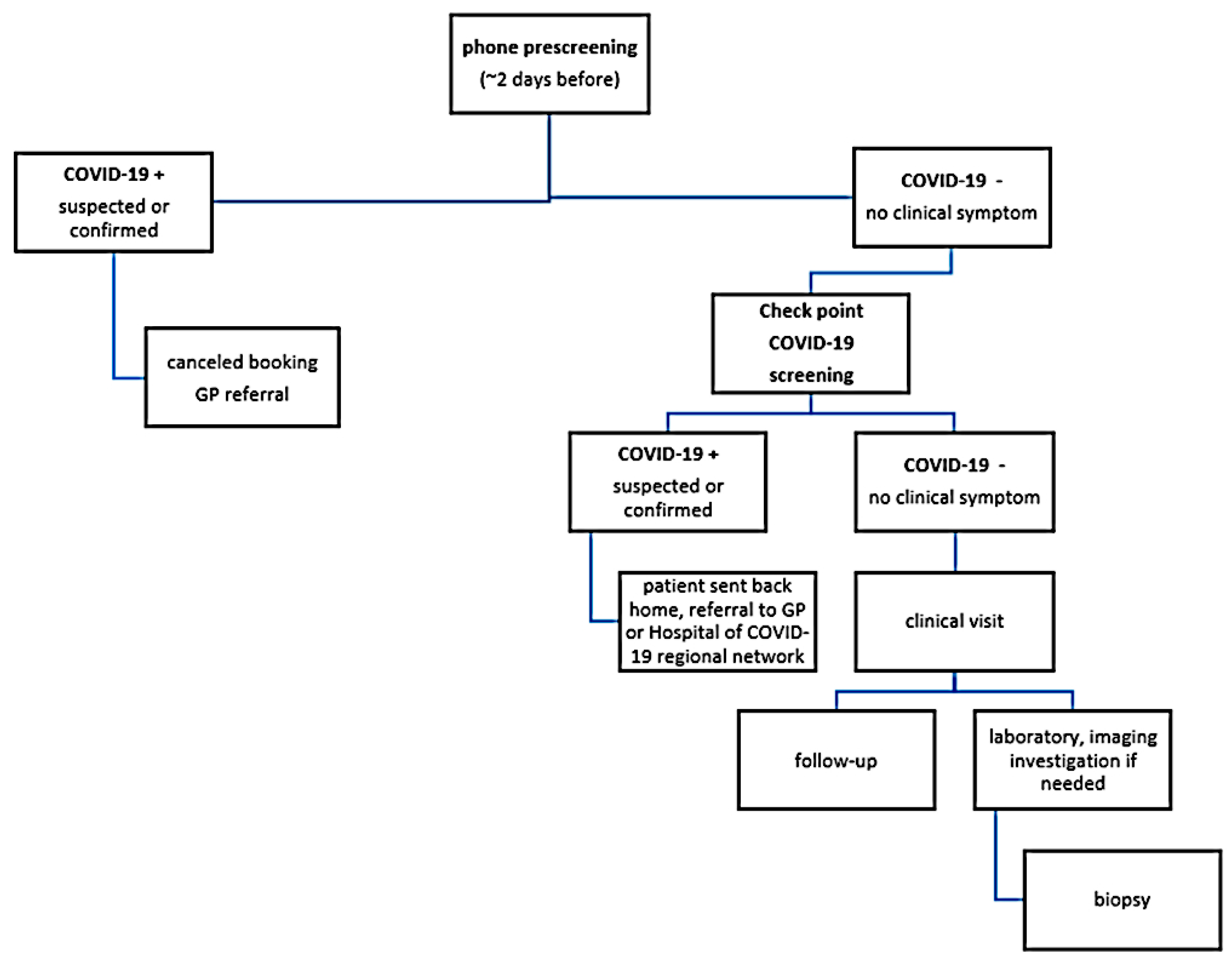
2.3.6. The Out-Patient Clinic
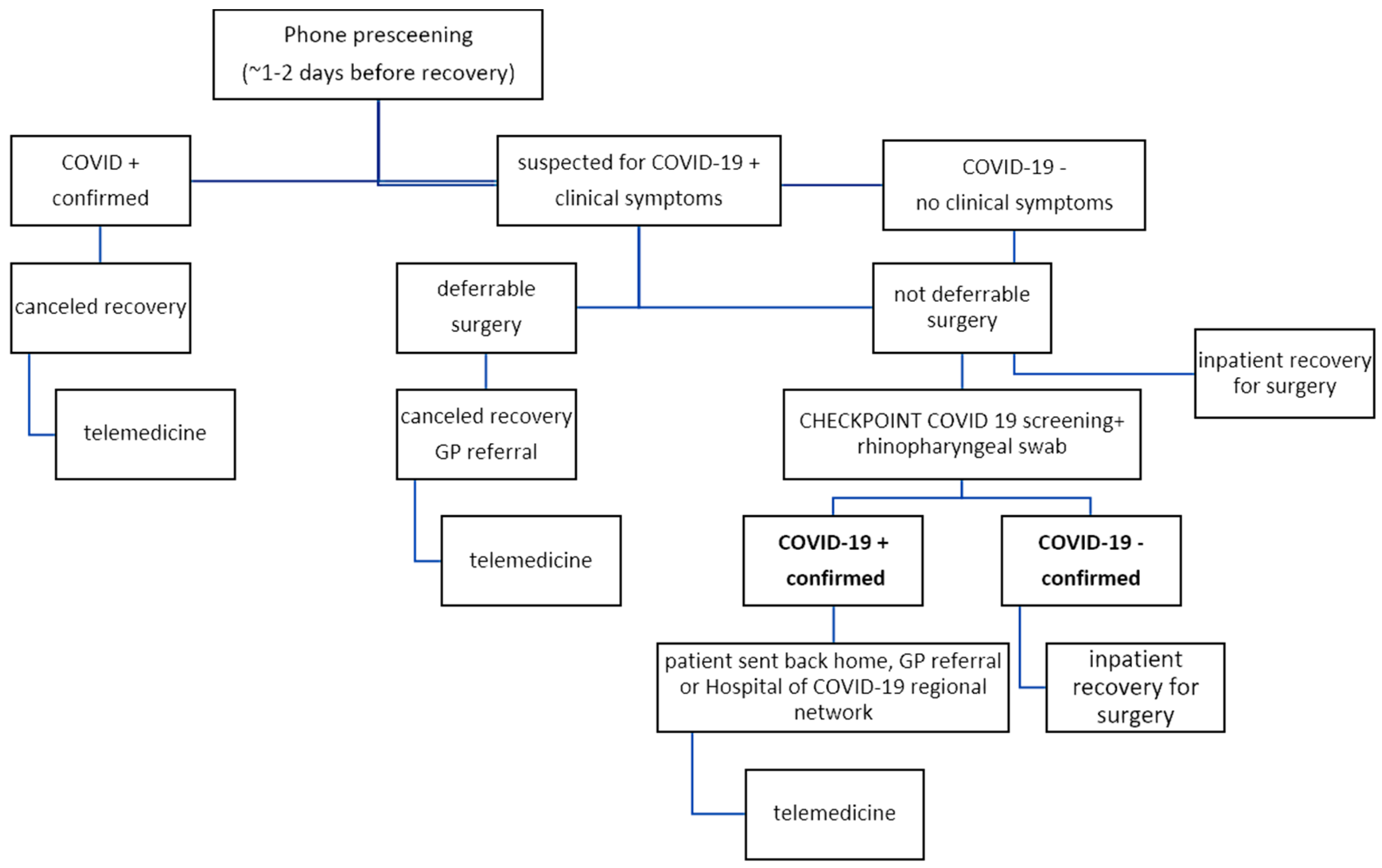
2.3.7. Wards and Surgery
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Decreto del Presidente del Consiglio dei Ministri, G.U. Serie Generale, n° 64, 11 March 2020. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/11/20A01605/sg (accessed on 19 April 2020).
- Coronavirus: Al via la Terza Fase Dell’Emergenza COVID-19. Available online: http://www.regione.lazio.it/rl/coronavirus/al-via-la-terza-fase-dellemergenza-covid-19/ (accessed on 19 April 2020).
- Liang, Z.C.; Wang, W.; Murphy, D.; Po Hui, J.H. Novel Coronavirus and orthopaedic surgery. Early experiences from Singapore. J. Bone Jt. Surg. Am. 2020, 102, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Capanna, F.; Haydar, A.; McCarey, C.; Bernini Carri, E.; Bartha Rasero, J.; Tsibizova, V.; Helmer, H.; Makatsarya, A.; Di Renzo, G.C. Preparing an obstetric unit in the heart of the epidemic strike of COVID-19: Quick reorganization tips. J. Matern. Fetal Neonatal Med. 2020, 12, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarac, N.J.; Sarac, B.A.; Schoenbrunner, A.R.; Janis, J.E.; Harrison, R.K.; Phieffer, L.S.; Quatman, C.E.; Ly, T.V. A Review of state guidelines for elective orthopaedic procedures during the COVID-19 outbreak. J. Bone Jt. Surg. Am. 2020, 102, 942–945. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; et al. Soft tissue and visceral sarcomas: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 268–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ZIP Folder with List ERN Members Per Country. Available online: https://metab.ern-net.eu/european-commission-and-erns/ (accessed on 20 April 2020).
- Monitoring from Ministry of Health. Available online: https://www.salute.gov.it/ (accessed on 9 April 2020).
- Legislative Decree 16 October 2003, n°288. Riordino Della Disciplina Degli Istituti di Ricovero e Cura a Carattere Scientifico. Art. 42, Comma 1, n° 3. 16 January 2003. Available online: https://www.gazzettaufficiale.it/eli/id/2003/10/27/003G0314/sg (accessed on 21 April 2020).
- Ministerial Decree 14 March 2013. “Documentazione Necessaria Per il Riconoscimento Degli Istituti di Ricovero e Cura a Carattere Scientifico”. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2013-06-27&atto.codiceRedazionale=13A05488&elenco30giorni (accessed on 21 April 2020).
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Stahl, J.P. CoVid19: Summary of Knowledge and Reliable Information Sources. UEMS Infect. Dis. Section. 26 March 2020. Available online: https://www.uems.eu/news-and-events/news/news-more/covid-19-update-from-uems (accessed on 21 April 2020).
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. 2020, e200980, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrantonio, F.; Garassino, M.C. Caring for patients with cancer during the COVID-19 outbreak in Italy. JAMA Oncol. 2020, 10, 821–822. [Google Scholar] [CrossRef] [PubMed]
- Delibera ifo_058.IFO_AOO.REGISTRO UFFICIALE.I.0005572.20-04-2020. Available online: https://www.ifo.it/delibera/ (accessed on 21 April 2020).
- Delibera ifo_058.IFO_AOO.REGISTRO UFFICIALE.U.0005348.14-04-2020. Available online: https://www.ifo.it/delibera/ (accessed on 21 April 2020).
- Ueda, M.; Martins, R.; Hendrie, P.C.; McDonnell, T.; Crews, J.R.; Wong, T.L.; McCreery, B.; Jagels, B.; Crane, A.; Byrd, D.R.; et al. Managing cancer care during the COVID-19 pandemic: Agility and collaboration toward a common goal. J. Natl. Compr. Canc. Netw. 2020, 18, 366–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capanna, R.; Piccioli, A.; Di Martino, A.; Daolio, P.A.; Ippolito, V.; Maccauro, G.; Piana, R.; Ruggieri, P.; Gasbarrini, A.; Spinelli, M.S.; et al. Management of long bone metastases: Recommendations from the Italian Orthopaedic Society bone metastasis study group. Expert. Rev. Anticancer. Ther. 2014, 14, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Henderson, E.R.; Groundland, J.S.; Pala, E.; Dennis, J.A.; Wooten, R.; Cheong, D.; Windhager, R.; Kotz, R.I.; Mercuri, M.; Funovics, P.T.; et al. Failure mode classification for tumor endoprostheses: Retrospective review of five institutions and a literature review. J. Bone Jt. Surg. Am. 2011, 93, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Cinar, P.; Kubal, T.; Freifeld, A.; Mishra, A.; Shulman, L.; Bachman, J.; Fonseca, R.; Uronis, H.; Klemanski, D.; Slusser, K.; et al. Safety at the time of the COVID-19 pandemic: How to keep our oncology patients and healthcare workers safe. J. Natl. Compr. Canc. Netw. 2020, 15, 1–6, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and multiorgan response. Curr. Probl. Cardiol. 2020, 45, 100618, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- ESMO-EURACAN Management and Treatment Adapted Recommendations in the COVID-19 Era: Sarcomas. Available online: https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic/sarcomas-in-the-covid-19-era (accessed on 7 June 2020).
- Available online: https://www.ifo.it/2020/04/22/nuovo-coronavirus-cosa-ce-da-sapere-come-proteggermi/ (accessed on 21 April 2020).
- Piqueras, M.; Marco, E.; Coll, M.; Escalada, F.; Ballester, A.; Cinca, C.; Belmonte, R.; Muniesa, J.M. Effectiveness of an interactive virtual telerehabilitation system in patients after total knee arthoplasty: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 392–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
|
|
|
|
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, B.; Zoccali, C.; Baldi, J.; Scotto di Uccio, A.; Biagini, R.; De Luca, A.; Petrongari, M.G.; Ferraresi, V. Reorganization Tips from a Sarcoma Unit at Time of the COVID-19 Pandemic in Italy: Early Experience from a Regional Referral Oncologic Center. J. Clin. Med. 2020, 9, 1868. https://doi.org/10.3390/jcm9061868
Rossi B, Zoccali C, Baldi J, Scotto di Uccio A, Biagini R, De Luca A, Petrongari MG, Ferraresi V. Reorganization Tips from a Sarcoma Unit at Time of the COVID-19 Pandemic in Italy: Early Experience from a Regional Referral Oncologic Center. Journal of Clinical Medicine. 2020; 9(6):1868. https://doi.org/10.3390/jcm9061868
Chicago/Turabian StyleRossi, Barbara, Carmine Zoccali, Jacopo Baldi, Alessandra Scotto di Uccio, Roberto Biagini, Assunta De Luca, Maria Grazia Petrongari, and Virginia Ferraresi. 2020. "Reorganization Tips from a Sarcoma Unit at Time of the COVID-19 Pandemic in Italy: Early Experience from a Regional Referral Oncologic Center" Journal of Clinical Medicine 9, no. 6: 1868. https://doi.org/10.3390/jcm9061868