Feasibility of Non-Gaussian Diffusion Metrics in Chronic Disorders of Consciousness

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
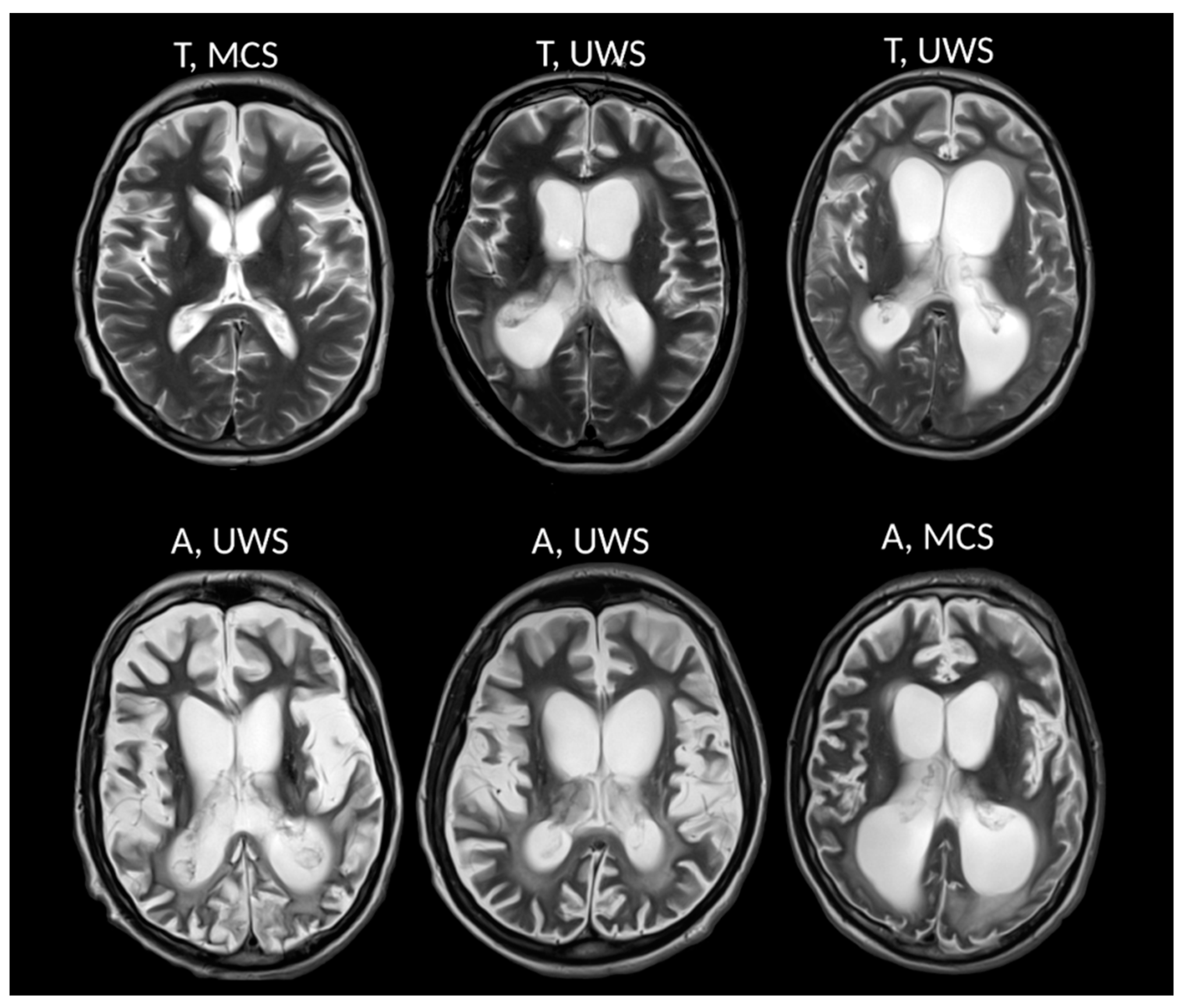
2.1. Patients
2.2. MRI Measurements
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
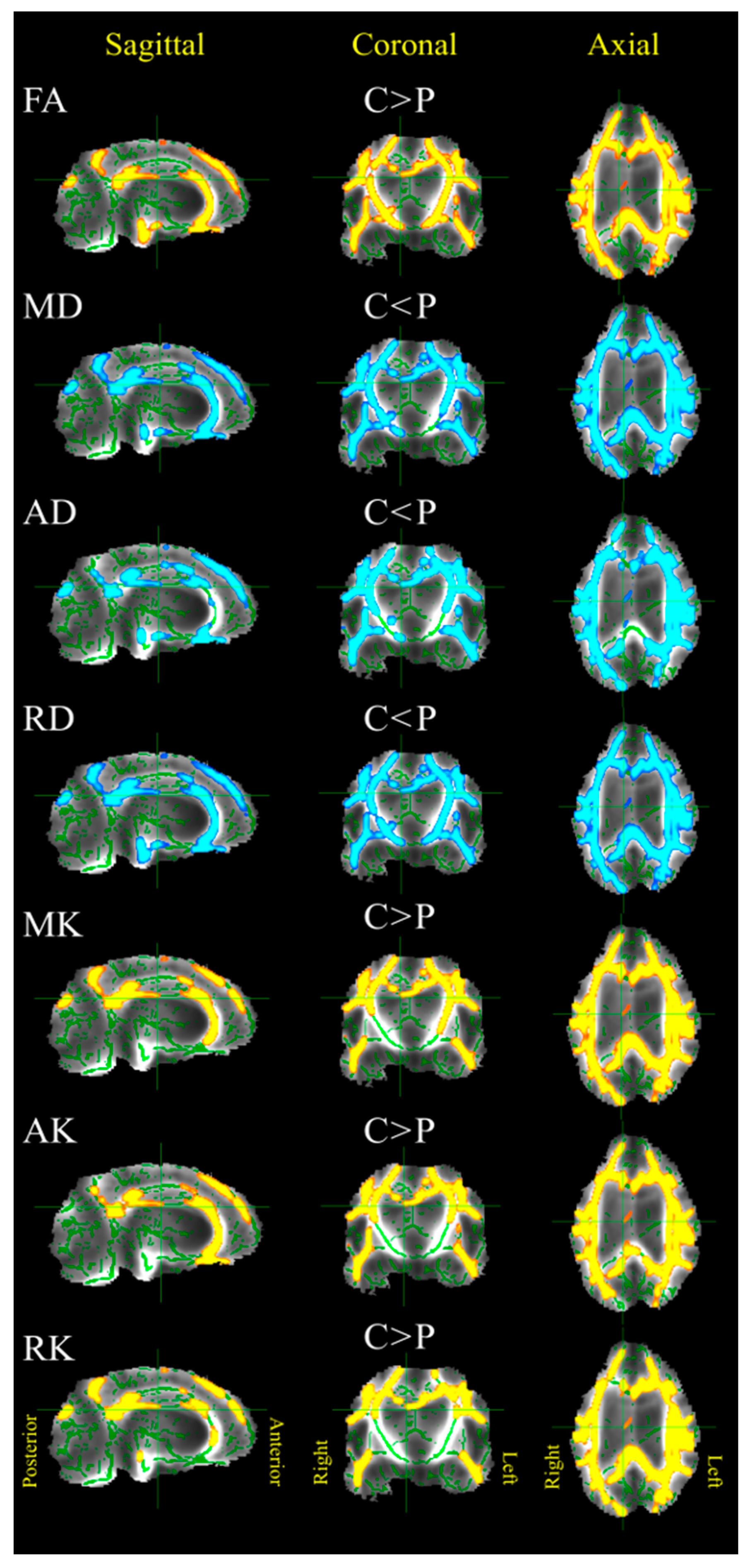
3.1. Patients versus Control Group
3.2. Anoxia versus Trauma Patient Groups
3.3. VS/UWS versus MCS Patients Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Laureys, S. The neural correlate of (un)awareness: Lessons from the vegetative state. Trends Cogn. Sci. 2005, 9, 556–559. [Google Scholar] [CrossRef]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef]
- Bernat, J.L. Chronic disorders of consciousness. Lancet 2006, 367, 1181–1192. [Google Scholar] [CrossRef]
- Schiff, N.D.; Fins, J.J. Brain death and disorders of consciousness. Curr. Biol. 2016, 26, R572–R576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Erp, W.; Larvrijsen, J.; Vos, P.; Bor, H.; Laureys, S.; Koopmans, R. The vegetative state: Prevalence, misdiagnosis and treatment limitations. JAMDA 2015, 85, 9–14. [Google Scholar] [CrossRef]
- Wannez, S.; Heine, L.; Thonnard, M.; Gosseries, O.; Laureys, S. The repetition of behavioral assessments in diagnosis of disorders of consciousness. Ann. Neurol. 2017, 81, 883–889. [Google Scholar] [CrossRef] [Green Version]
- Di Perri, C.; Thibaut, A.; Heine, L.; Soddu, A.; Demertzi, A.; Laureys, S. Measuring consciousness in coma and related states. World J. Radiol. 2014, 6, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodart, O.; Gosseries, O.; Wannez, S.; Thibaut, A.; Annen, J.; Boly, M.; Rosanova, M.; Casali, A.G.; Casarotto, S.; Tononi, G.; et al. Measures of metabolism and complexity in the brain of patients with disorders of consciousness. NeuroImage Clin. 2017, 14, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Stender, J.; Gosseries, O.; Bruno, M.-A.; Charland-Verville, V.; Vanhaudenhuyse, A.; Demertzi, A.; Chatelle, C.; Thonnard, M.; Thibaut, A.; Heine, L.; et al. Diagnostic precision of PET imaging and functional MRI in disorders of consciousness: A clinical validation study. Lancet 2014, 384, 514–522. [Google Scholar] [CrossRef]
- Jellinger, K.A. Neuropathology of prolonged unresponsive wakefulness syndrome after blunt head injury: Review of 100 post-mortem cases. Brain Inj. 2013, 27, 917–923. [Google Scholar] [CrossRef]
- Kinney, H.C.; Korein, J.; Panigraphy, A.; Dikkes, P.; Goode, R. Neuropathological findings in the brain of Karen Ann Quinlan. The role of thalamus in the persistent vegetative state. N. Engl. J. Med. 1994, 330, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Boly, M.; Tshibanda, L.; Vanhaudenhuyse, A.; Noirhomme, Q.; Schnakers, C.; Ledoux, D.; Boveroux, P.; Garweg, C.; Lambermont, B.; Phillips, C. Functional connectivity in the default network during resting state is preserved in a vegetative but not in a brain dead patient. Hum. Brain Mapp. 2009, 30, 2393–2400. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, N.; Okumura, A.; Shinoda, J.; Nakashima, T.; Iwama, T. Relationship between regional cerebral metabolism and consciousness disturbance in traumatic diffuse brain injury without large focal lesions: An FDG-PET study with statistical parametric mapping analysis. J. Neurol. Neurosurg. Psychiatry 2006, 77, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Alacoque, X.; Fourcade, O.; Samii, K.; Marque, P.; Woods, R.; Mazziotta, J.; Chollet, F.; Loubinoux, I. Wakefulness and loss of awareness: Brain and brainstem interaction in the vegetative state. Neurology 2010, 74, 313–320. [Google Scholar] [CrossRef]
- Di Perri, C.; Bahri, M.A.; Amico, E.; Thibaut, A.; Heine, L.; Antonopoulos, G.; Charland-Verville, V.; Wannez, S.; Gomez, F.; Hustinx, R.; et al. Neural correlates of consciousness in patients who have emerged from a minimally conscious state: A cross-sectional multimodal imaging study. Lancet Neurol. 2016, 15, 830–842. [Google Scholar] [CrossRef]
- Laureys, S.; Tononi, G. The Neurology of Consciousness; Academic Press-Elsevier: London, UK, 2008. [Google Scholar]
- Mashour, G.A.; Hudetz, A.G. Neural correlates of unconsciousness in large-scale brain networks trends. Neuroscience 2018, 41, 150–160. [Google Scholar] [CrossRef]
- Laouchedi, M.; Galanaud, D.; Delmaire, C.; Fernandez-Vidal, S.; Messé, A.; Mesmoudi, S.; Oulebsir Boumgharb, F.; Pélégrini-Issaca, M.; Puybasseta, L.; Benali, H.; et al. Deafferentation in thalamic and pontine areas in severe traumatic brain injury. J. Neuroradiol. 2015, 42, 202–211. [Google Scholar] [CrossRef]
- Kampfl, A.; Schmutzhard, E.; Franz, G.; Pfausler, B.; Haring, H.P.; Ulmer, H.; Felber, S.; Golaszewski, S.; Aichner, F. Prediction of recovery from post-traumatic vegetative state with cerebral magnetic-resonance imaging. Lancet 1998, 351, 1763–1767. [Google Scholar] [CrossRef]
- Hoelper, B.M.; Soldner, F.; Choné, L.; Wallenfang, T. Effect of intracerebral lesions detected in early MRI on outcome after acute brain injury. Acta Neurochir. 2000, 76, 265–267. [Google Scholar]
- Annen, J.; Heine, L.; Ziegler, E.; Frasso, G.; Bahri, M.; Di Perri, C.; Stender, J.; Martial, C.; Wannez, S.; D’ostilio, K.; et al. Function–structure connectivity in patients with severe brain injury as measured by MRI-DWI and FDG-PET. Hum. Brain Mapp. 2016, 37, 3707–3720. [Google Scholar] [CrossRef]
- Fernandez-Espejo, D.; Bekinschtein, T.; Monti, M.M.; Pickard, J.D.; Junque, C.; Coleman, M.R.; Owen, A.M. Diffusion weighted imaging distinguishes the vegetative state from the minimally conscious state. NeuroImage 2011, 54, 103–112. [Google Scholar] [CrossRef]
- Newcombe, V.F.; Williams, G.B.; Scoffings, D.; Cross, J.; Carpenter, T.A.; Pickard, J.D.; Menon, D.K. Aetiological differences in neuroanatomy of the vegetative state: Insights from diffusion tensor imaging and functional implications. J. Neurol. Neurosurg. Psychiatry 2010, 81, 552–561. [Google Scholar] [CrossRef]
- Zheng, Z.S.; Reggente, N.; Lutkenhoff, E.; Owen, A.M.; Monti, M.M. Disentangling disorders of consciousness: Insights from diffusion tensor imaging and machine learning. Hum. Brain Mapp. 2017, 38, 431–443. [Google Scholar] [CrossRef]
- Velly, L.; Perlbarg, V.; Boulier, T.; Adam, N.; Delphine, S.; Luyt, C.-E.; Battisti, V.; Torkomian, G.; Arbelot, C.; Chabanne, R.; et al. Use of brain diffusion tensor imaging for the prediction of long-term neurological outcomes in patients after cardiac arrest: A multicentre, international, prospective, observational, cohort study. Lancet Neurol. 2018, 17, 317–326. [Google Scholar] [CrossRef]
- Van der Eerden, A.W.; Khalilzadeh, O.; Perlbarg, V.; Dinkel, J.; Sanchez, P.; Vos, P.E.; Luyt, C.E.; Stevens, R.D.; Menjot de Champfleur, N.; Delmaire, C.; et al. White Matter Changes in Comatose Survivors of Anoxic Ischemic Encephalopathy and Traumatic Brain Injury: Comparative Diffusion-Tensor Imaging Study. Radiology 2014, 270, 506–516. [Google Scholar] [CrossRef]
- Dinkel, J.; Drier, A.; Khalilzadeh, O.; Perlbarg, V.; Czernecki, V.; Gupta, R.; Gomas, F.; Sanchez, P.; Dormont, D.; Galanaud, D.; et al. Long-Term White Matter Changes after Severe Traumatic Brain Injury: A 5-Year Prospective Cohort. Am. J. Neuroradiol. 2013, 35, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Basser, P.J.; Jones, D.K. Diffusion-tensor MRI: Theory, experimental design and data analysis—A technical review. NMR Biomed. 2002, 15, 456–467. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A.; Ramani, A.; Lu, H.; Kaczynski, K. Diffusional kurtosis imaging: The quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn. Reson. Med. 2005, 53, 1432–1440. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010, 23, 698–710. [Google Scholar] [CrossRef]
- Vellmer, S.; Tonoyan, A.S.; Suter, D.; Pronin, I.N.; Maximov, I.I. Validation of DWI pre-processing procedures for reliable differentiation between human brain gliomas. Z. Med. Phys. 2018, 28, 14–24. [Google Scholar] [CrossRef]
- De Santis, S.; Bastiani, M.; Droby, A.; Kolber, P.; Zipp, F.; Pracht, E.; Stoecker, T.; Groppa, S.; Roebroeck, A. Characterizing Microstructural Tissue Properties in Multiple Sclerosis with Diffusion MRI at 7 T and 3 T: The Impact of the Experimental Design. Neuroscience 2018, 403, 17–26. [Google Scholar] [CrossRef]
- Maximov, I.I.; Tonoyan, A.S.; Pronin, I.N. Differentiation of glioma malignancy grade using diffusion MRI. Phys. Med. 2017, 40, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Grinberg, F.; Maximov, I.I.; Farrher, E.; Neuner, I.; Amort, L.; Thönneßen, H.; Oberwelland, E.; Konrad, K.; Shah, N.J. Diffusion kurtosis metrics as biomarkers of microstructural development: A comparative study of a group of children and a group of adults. NeuroImage 2017, 44, 12–22. [Google Scholar] [CrossRef]
- Porcari, P.; Hegi, M.E.; Lei, H.; Hamou, M.F.; Vassallo, I.; Capuani, S.; Gruetter, R.; Mlynarik, V. Early detection of human glioma sphere xenografts in mouse brain using diffusion MRI at 14.1 T: Early detection of glioma xenografts using diffusion MRI at 14.1 T. NMR Biomed. 2016, 29, 1577–1589. [Google Scholar] [CrossRef]
- Steven, A.J.; Zhuo, J.; Melhem, E.R. Diffusion kurtosis imaging: An emerging technique for evaluating the microstructural environment of the brain. Am. J. Roentgenol. 2014, 202, 26–33. [Google Scholar] [CrossRef]
- Cheung, J.S.; Wang, E.; Lo, E.H.; Sun, P.Z. Stratification of heterogeneous diffusion MRI ischemic lesion with kurtosis imaging. Stroke 2012, 43, 2252–2254. [Google Scholar] [CrossRef]
- Surova, Y.; Nilsson, M.; Lampinen, B.; Lätt, J.; Hall, S.; Widner, H.; van Westen, D.; Hansson, O. Alteration of putaminal fractional anisotropy in Parkinson’s disease: A longitudinal diffusion kurtosis imaging study. Neuroradiology 2018, 60, 247–254. [Google Scholar] [CrossRef]
- Kamagata, K.; Zalesky, A.; Hatano, T.; Ueda, R.; Di Biase, M.A.; Okuzumi, A.; Shimoji, K.; Hori, M.; Caeyenberghs, K.; Pantelis, C.; et al. Gray Matter Abnormalities in Idiopathic Parkinson’s Disease: Evaluation by Diffusional Kurtosis Imaging and Neurite Orientation Dispersion and Density Imaging. Hum. Brain Mapp. 2017, 38, 3704–3722. [Google Scholar] [CrossRef]
- Van Cauter, S.; Veraart, J.; Sijbers, J.; Peeters, R.R.; Himmelreich, U.; De Keyzer, F.; van Gool, S.W.; van Calenbergh, F.; de Vleeschouwer, S.; van Hecke, W.; et al. Gliomas: Diffusion kurtosis MR imaging in grading. Radiology 2012, 263, 492–501. [Google Scholar] [CrossRef]
- Falangola, M.F.; Guilfoyle, D.N.; Tabesh, A.; Hui, E.S.; Nie, X.; Jensen, J.H.; Gerum, S.V.; Hu, C.; La Francois, J.; Collins, H.R.; et al. Histological Correlation of Diffusional Kurtosis and White Matter Modeling Metrics in the Cuprizone-Induced Corpus Callosum Demyelination. NMR Biomed. 2014, 27, 948–957. [Google Scholar] [CrossRef]
- Seel, R.T.; Sherer, M.; Whyte, J.; Katz, D.I.; Giacino, J.T.; Rosenbaum, A.M.; Hammond, F.M.; Kalmar, K.; Pape, T.L.; Zafonte, R.; et al. Assessment scales for disorders of consciousness: Evidence-based recommendations for clinical practice and research. Arch. Phys. Med. Rehabil. 2010, 91, 1795–1813. [Google Scholar] [CrossRef]
- Aja-Fernández, S.; Tristán-Vega, A.; Hoge, S. Statistical noise analysis in GRAPPA using a parametrized non-central chi approximation model. Magn. Reson. Med. 2011, 65, 1195–1206. [Google Scholar] [CrossRef]
- Andersson, J.; Sotiropoulos, S. An integrated approach to correction for offresonance effects and subject movement in diffusion MR imaging. Neuroimage 2016, 125, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Leemans, A.; Jones, D. The b-matrix must be rotated when correcting for subject motion in DTI data. Magn. Reson. Med. 2009, 62, 1336–1349. [Google Scholar] [CrossRef] [PubMed]
- Veraart, J.; Fieremans, E.; Jelescu, I.; Knoll, F.; Novikov, D.S. Gibbs ringing in diffusion MRI. Magn. Reson. Med. 2016, 76, 301–314. [Google Scholar] [CrossRef]
- Maximov, I.I.; Thönneßen, H.; Konrad, K.; Amort, L.; Neuner, I.; Shah, N.J. Statistical instability of TBSS analysis based on DTI fitting algorithm. J. Neuroimaging 2015, 25, 883–891. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D. ExploreDTI: A graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc. Intl. Soc. Magn. Reson. Med. 2009, 17, 3537. [Google Scholar]
- Poot, D.H.; den Dekker, A.J.; Achten, E.; Verhoye, M.; Sijbers, J. Optimal experimental design for diffusion kurtosis imaging. IEEE Trans. Med. Imaging 2010, 29, 819–829. [Google Scholar] [CrossRef]
- Lanzafame, S.; Giannelli, M.; Garaci, F.; Floris, R.; Duggento, A.; Guerrisi, M.; Toschi, N. Differences in Gaussian diffusion tensor imaging and non-Gaussian diffusion kurtosis imaging model-based estimates of diffusion tensor invariants in the human brain. Med. Phys. 2016, 43, 2464. [Google Scholar] [CrossRef]
- Zhang, Y.; Brady, M.; Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans. Med. Imaging 2001, 20, 45–57. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- Bodart, O.; Amico, E.; Gómez, F.; Casali, A.G.; Wannez, S.; Heine, L.; Thibaut, A.; Annen, J.; Boly, M.; Casarotto, S.; et al. Global structural integrity and effective connectivity in patients with disorders of consciousness. Brain Stimul. 2017, 11, 358–365. [Google Scholar] [CrossRef]
- Kinney, H.C.; Samuels, M.A. Neuropathology of the persistent vegetative state. A review. J. Neuropath. Exp. Neurol. 1994, 53, 548–558. [Google Scholar] [CrossRef]
- Helpern, J.A.; Adisetiyo, V.; Falangola, M.F.; Hu, C.; Di Martino, A.; Williams, K.; Castellanos, F.X.; Jensen, J.H. Preliminary evidence of altered gray and white matter microstructural development in the frontal lobe of adolescents with attention-deficit hyperactivity disorder: A diffusional kurtosis imaging study. J. Magn. Reson. Imaging 2011, 33, 17–23. [Google Scholar] [CrossRef]
- Lu, H.; Jensen, J.H.; Ramani, A.; Helpern, J.A. Three-dimensional characterization of non-gaussian water diffusion in humans using diffusion kurtosis imaging. NMR Biomed. 2006, 19, 236–247. [Google Scholar] [CrossRef]
- Raab, P.; Hattingen, E.; Franz, K.; Zanella, F.E.; Lanfermann, H. Cerebral gliomas: Diffusional kurtosis imaging analysis of microstructural differences. Radiology 2010, 254, 876–881. [Google Scholar] [CrossRef]
- Ramani, A.; Jensen, J.H.; Szulc, K.U.; Ali, O.; Hu, C.; Lu, H.; Brodle, J.D.; Helpern, J.A. Assessment of Abnormalities in the Cerebral Microstructure of Schizophrenia Patients: A Diffusional Kurtosis Imaging Study. Proc. Int. Soc. Magn. Reson. Med. 2007, 15, 648. [Google Scholar]
- Grossman, E.J.; Ge, Y.; Jensen, J.H.; Babb, J.S.; Miles, L.; Reaume, J.; Silver, J.M.; Grossman, R.I.; Inglese, M. Thalamus and Cognitive Impairment in Mild Traumatic Brain Injury: A Diffusional Kurtosis Imaging Study. J. Neurotrauma 2012, 29, 2318–2327. [Google Scholar] [CrossRef]
- Yu, F.; Shukla, D.K.; Armstrong, R.C.; Marion, C.M.; Radomski, K.L.; Selwyn, R.G.; Dardzinski, B.J. Repetitive Model of Mild Traumatic Brain Injury Produces Cortical Abnormalities Detectable by Magnetic Resonance Diffusion Imaging, Histopathology, and Behavior. J. Neurotrauma 2017, 34, 1364–1381. [Google Scholar] [CrossRef] [Green Version]
- Sours, C.; Raghavan, P.; Medina, A.E.; Roys, S.; Jiang, L.; Zhuo, J.; Gullapalli, R.P. Structural and Functional Integrity of the Intraparietal Sulcus in Moderate and Severe Traumatic Brain Injury. J. Neurotrauma 2017, 34, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Stokum, J.A.; Sours, C.; Zhuo, J.; Kane, R.; Shanmuganathan, K.; Gullapalli, R.P. A longitudinal evaluation of diffusion kurtosis imaging in patients with mild traumatic brain injury. Brain Inj. 2015, 29, 47–57. [Google Scholar] [CrossRef]
- Adams, J.H.; Graham, D.I.; Jennett, B. The neuropathology of the vegetative state after an acute brain insult. Brain 2000, 123, 1327–1338. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.I. Pathology of hypoxic brain damage in man. J. Clin. Path. 1977, 30, 170–180. [Google Scholar] [CrossRef]
- Maxwell, W.L.; Dhillon, K.; Harper, L.; Espin, J.; MacIntosh, T.K.; Smith, D.H.; Graham, D.I. There is differential loss of pyramidal cells from the human hippocampus with survival after blunt head injury. J. Neuropathol. Exp. Neurol. 2003, 62, 272–279. [Google Scholar] [CrossRef]
- Feldman, H.M.; Yeatman, J.D.; Lee, E.S.; Barde, L.H.; Gaman-Bean, S. Diffusion Tensor Imaging: A Review for Pediatric Researchers and Clinicians. J. Dev. Behav. Pediatr. 2010, 31, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.L.; Hurley, S.A.; Samsonov, A.A.; Adluru, N.; Hosseinbor, A.P.; Mossahebi, P.; Tromp do, P.M.; Zakszewski, E.; Field, A.S. Characterization of Cerebral White Matter Properties Using Quantitative Magnetic Resonance Imaging Stains. Brain Connect. 2011, 1, 423–446. [Google Scholar] [CrossRef]
- Wheeler–Kingshott, C.A.M.; Cercignani, M. About “axial” and “radial” diffusivities. Magn. Reson. Med. 2009, 61, 1255–1260. [Google Scholar] [CrossRef]
- Field, A.S.; Alexander, A.L.; Wu, Y.C.; Hasan, K.M.; Witwer, B.; Badie, B. Diffusion tensor eigenvector directional color imaging patterns in the evaluation of cerebral white matter tracts altered by tumor. J. Magn. Reson. Imaging 2004, 20, 555–562. [Google Scholar] [CrossRef]
- Zhuo, J.; Xu, S.; Proctor, J.L.; Mullins, R.J.; Simon, J.Z.; Fiskum, G.; Gullapalli, R.P. Diffusion kurtosis as an in vivo imaging marker for reactive astrogliosis in traumatic brain injury. Neuroimage 2012, 59, 467–477. [Google Scholar] [CrossRef] [Green Version]
- Cavaliere, C.; Aiello, M.; Di Perri, C.; Fernandez-Espejo, D.; Owen, A.M.; Soddu, A. Diffusion tensor imaging and white matter abnormalities in patients with disorders of consciousness. Front. Hum. Neurosci. 2015, 8, 1028. [Google Scholar] [CrossRef] [PubMed]
- Maximov, I.I.; Alnaes, D.; Westlye, L.T. Towards an Optimised Processing Pipeline for Diffusion MRI Data: Effects of Artefact Corrections on Diffusion Metrics and Their Age Associations in UK Biobank. Available online: https://www.biorxiv.org/content/10.1101/511964v1.abstract (accessed on 26 May 2019).
- Bammer, R.; Holdsworth, S.J.; Veldhuis, W.B.; Skare, S.T. New methods in Diffusion Weighted and Diffusion Tensor Imaging. Magn. Reson. Imaging Clin. N. Am. 2009, 17, 175–204. [Google Scholar] [CrossRef] [PubMed]
- Mac Donald, C.L.; Dikranian, K.; Bayly, P.; Holtzman, D.; Brody, D. Diffusion Tensor Imaging Reliably Detects Experimental Traumatic Axonal Injury and Indicates Approximate Time of Injury. J. Neurosci. 2007, 27, 11869–11876. [Google Scholar] [CrossRef] [PubMed]
- Edlow, B.L.; Haynes, R.L.; Takahashi, E.; Klein, J.P.; Cummings, P.; Benner, T.; Greer, D.M.; Greenberg, S.M.; Wu, O.; Kinney, H.C.; et al. Disconnection of the Ascending Arousal System in Traumatic Coma. J. Neuropathol. Exp. Neurol. 2013, 72, 505–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Sex | Age | MPI | CRS-R | Aetiology | Lesion Site | Diagnosis |
|---|---|---|---|---|---|---|---|
| 1 | M | 20 | 15 | 21 | T | B | MCS |
| 2 | M | 48 | 13 | 7 | A | L > R | VS/UWS |
| 3 | F | 47 | 26 | 5 | A | L > R | VS/UWS |
| 4 | F | 31 | 5 | 18 | A | L > R | MCS |
| 5 | M | 23 | 5 | 6 | A | B | VS/UWS |
| 6 | M | 26 | 5 | 12 | T | B | MCS |
| 7 | F | 24 | 22 | 7 | T | B | VS/UWS |
| 8 | M | 23 | 12 | 12 | T | L > R | MCS |
| 9 | M | 47 | 9 | 12 | A | B | MCS |
| 10 | M | 22 | 12 | 5 | T | B | VS/UWS |
| 11 | F | 25 | 12 | 7 | T | B | VS/UWS |
| 12 | M | 67 | 7 | 6 | A | B | VS/UWS |
| 13 | M | 47 | 30 | 6 | A | B | VS/UWS |
| 15 | F | 43 | 7 | 13 | A | R > L | MCS |
| 15 | M | 51 | 16 | 5 | A | B | VS/UWS |
| 16 | F | 24 | 73 | 4 | A | B | VS/UWS |
| 17 | M | 33 | 10 | 12 | A | R > L | MCS |
| 18 | M | 42 | 3 | 6 | A | L > R | VS/UWS |
| FA | MD (µm2/ms) | AD (µm2/ms) | RD (µm2/ms) | MK | AK | RK | |
|---|---|---|---|---|---|---|---|
| GM | C < P | C < P | C < P | C > P | C > P | C > P | |
| Control | 1.5/0.10 | 1.6/0.11 | 1.4/0.10 | 0.66/0.05 | 0.63/0.03 | 0.66/0.04 | |
| Patient | 2.1/0.45 | 2.3/0.46 | 2.0/0.45 | 0.58/0.25 | 0.52/0.09 | 0.59/0.23 | |
| Cohen’s d | 1.97 | 2.05 | 1.91 | −0.4 | −1.6 | −0.39 | |
| WM | C > P | C < P | C < P | C < P | C > P | C > P | C > P |
| Control | 0.28/0.01 | 1.0/0.08 | 1.3/0.08 | 0.9/0.09 | 0.87/0.05 | 0.76/0.04 | 0.70/0.07 |
| Patient | 0.17/0.03 | 1.6/0.40 | 1.9/0.38 | 1.5/0.41 | 0.68/0.22 | 0.64/0.14 | 0.98/0.24 |
| Cohen’s d | −3.28 | 1.99 | 1.86 | 2.07 | −1.13 | −1.19 | −1.51 |
| Brainstem | C > P | C < P | C < P | C < P | C > P | C > P | |
| Control | 0.32/0.10 | 1.4/0.19 | 1.8/0.23 | 1.1/0.15 | 0.85/0.13 | 0.76/0.12 | |
| Patient | 0.22/0.04 | 1.9/0.25 | 2.3/0.31 | 1.7/0.26 | 0.75/0.09 | 0.68/0.06 | |
| Cohen’s d | −4.66 | 3.03 | 3.06 | 3.06 | −1.5 | −2.05 | |
| Thalamus | C < P | C < P | C < P | ||||
| Control | 1.2/0.20 | 1.4/0.23 | 1.0/0.20 | ||||
| Patient | 1.7/0.33 | 2.0/0.33 | 1.5/0.33 | ||||
| Cohen’s d | 2.31 | 2.7 | 2.17 | ||||
| CC | C > P | C < P | C < P | C < P | C > P | C > P | C > P |
| Control | 0.44/0.12 | 1.5/0.17 | 2.2/0.31 | 1.1/0.18 | 0.94/0.13 | 0.62/0.04 | 1.28/0.25 |
| Patient | 0.20/0.08 | 2.2/0.42 | 2.6/0.36 | 2.0/0.46 | 0.58/0.12 | 0.52/0.05 | 0.60/0.14 |
| Cohen’s d | −4.46 | 2.21 | 1.42 | 2.5 | −4.17 | −2.47 | −7.52 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kremneva, E.I.; Legostaeva, L.A.; Morozova, S.N.; Sergeev, D.V.; Sinitsyn, D.O.; Iazeva, E.G.; Suslin, A.S.; Suponeva, N.A.; Krotenkova, M.V.; Piradov, M.A.; et al. Feasibility of Non-Gaussian Diffusion Metrics in Chronic Disorders of Consciousness. Brain Sci. 2019, 9, 123. https://doi.org/10.3390/brainsci9050123
Kremneva EI, Legostaeva LA, Morozova SN, Sergeev DV, Sinitsyn DO, Iazeva EG, Suslin AS, Suponeva NA, Krotenkova MV, Piradov MA, et al. Feasibility of Non-Gaussian Diffusion Metrics in Chronic Disorders of Consciousness. Brain Sciences. 2019; 9(5):123. https://doi.org/10.3390/brainsci9050123
Chicago/Turabian StyleKremneva, Elena I., Liudmila A. Legostaeva, Sofya N. Morozova, Dmitry V. Sergeev, Dmitry O. Sinitsyn, Elizaveta G. Iazeva, Aleksandr S. Suslin, Natalia A. Suponeva, Marina V. Krotenkova, Michael A. Piradov, and et al. 2019. "Feasibility of Non-Gaussian Diffusion Metrics in Chronic Disorders of Consciousness" Brain Sciences 9, no. 5: 123. https://doi.org/10.3390/brainsci9050123