
Abstract
Long-term recovery of volitional control of the upper limb is a major unmet need in people with paralysis. Recently, it has been demonstrated that spinal cord stimulation, when paired with intense physical therapy, can restore volitional control of upper limb in spinal cord injury (SCI). Epidural stimulation of the spinal cord has traditionally been demonstrated to be highly effective in restoring movement, potentially due to the ability of targeted activation of specific motoneuron pools. However, transcutaneous spinal cord stimulation (tSCS) has recently shown equally promising results. In this study, we use a custom designed electrode patch and stimulator to enable targeted stimulation of specific spinal segments. We show that targeted transcutaneous stimulation of the cervical spinal cord can substantially and rapidly improve volitionally evoked muscle activity and force, even with minimal physical therapy, in two individuals with SCI. We also show, for the first time, the effectiveness of tSCS in restoring strength and dexterity in an individual with paralysis of the hand due to a peripheral injury.
Introduction
Spinal cord and peripheral injury can result in paralysis due to the disruption in the transmission of neural signals. More than half of spinal cord injuries (SCIs) occur at the cervical level (NSCISC and University of Alabama at Birmingham, 2021), and regaining voluntary control of the hand and arm is the highest priority in such cases (Anderson, 2004). However, the chances of regaining hand and arm function are exceedingly low beyond 12-18 months post injury (Fawcett et al., 2006).
Electrical stimulation of the lumbar spinal cord using epidurally placed electrodes has recently shown great promise in being able to evoke voluntary movements of the lower limb during stimulation after SCI, in rats (van den Brand et al., 2012), non-human primates (Capogrosso et al., 2016) and humans (Harkema et al., 2011; Angeli et al., 2014, 2018; Gill et al., 2018; Wagner et al., 2018). Additionally, when paired with intense motor training, lumbar epidural stimulation has also demonstrated persistent increase in voluntary control of the lower limbs even in the absence of stimulation (Rejc et al., 2017; Angeli et al., 2018; Wagner et al., 2018). Epidural stimulation has been shown to primarily engage the large-to-medium size sensory afferent fibers present in the dorsal column and roots of the spinal cord (Rattay et al., 2000). Local spinal circuits constitute of these afferent fibers forming synaptic connections with spinal interneurons and motoneurons. Pharmacological and computational experiments (Capogrosso et al., 2013) suggest that activation of the dorsal fibers increases the excitability of the local spinal circuitry including the efferent fibers. Expanding this idea further, recent studies have demonstrated that epidural stimulation targeted at the cervical spinal cord could activate (Greiner et al., 2020) and restore upper limb movement (Lu et al., 2016). Though extremely promising, the invasive nature of epidural stimulation is a major hurdle for clinical translation and long-term rehabilitation (James et al., 2018; Taccola et al., 2020).
Meanwhile, non-invasive, persistent stimulation of the spinal cord using transcutaneous electrodes has been demonstrated to evoke voluntary movements in both upper (Freyvert et al., 2018; Gad et al., 2018; Inanici et al., 2021) and lower limbs (Sayenko et al., 2015, 2019). Moreover, recent evidence suggests that transcutaneous spinal cord stimulation (tSCS), like epidural stimulation, exerts its neuromodulatory effect on motoneurons trans-synaptically via activation of large-to-medium size sensory afferent fibers (Ladenbauer et al., 2010; Hofstoetter et al., 2018) and can also enhance supraspinal inputs (Guiho et al., 2021). Only recently, has it been shown that pairing tSCS at the cervical levels with intense motor training can result in sustained improvements in hand and arm function (Benavides et al., 2020; Zhang et al., 2020; Inanici et al., 2021). Taken together, tSCS can be a promising rehabilitative tool for people with SCI.
A few technical limitations limit the effectiveness of tSCS. The commercially available electrodes used for tSCS are relatively large, thereby limiting the precision in which stimulation can be delivered to cervical targets for evoking upper-limb activity. By virtue of being placed over the skin, the electrodes are also relatively far from the dorsal fibers of the spinal cord with layers of intervening connective and bony tissue including the dorsal aspects of the cervical vertebrae. This limits the effectiveness and specificity in the recruitment of the different motoneuron pools which could be a major drawback for tSCS, as epidural stimulation studies shown the importance of targeted stimulation (Wagner et al., 2018) in restoring voluntary muscle control.
We performed targeted transcutaneous stimulation of the cervical spinal cord paired with minimal physical therapy in two individuals classified as having a motor complete SCI and one individual with a peripheral nerve injury. Stimulation was targeted to specific cervical levels using a custom electronically configurable electrode array, with each electrode having a small form factor (10 mm x 10 mm). Modulating the spatial configuration of the stimulation electronically allowed us to extensively map the recruitment profile of the upper-limb muscles based on the location of stimulation. This enabled us to choose the precise location of stimulation to achieve maximal recruitment of the muscle group of interest. Even though participants received stimulation only once per week, we observed a rapid increase in both volitionally controlled muscle activity and effective force within a period of 5-6 weeks.
However, the observed gains were restricted to muscles that generated at least a measurable amount of force at the beginning of therapy. In the subject with peripheral nerve injury leading to paralysis of the hand, we observed rapid increase in functionality of the affected digits.
Taken together, this study describes the advantages of using a highly configurable electrode array and even minimal physical therapy in restoring volitional control of upper-limb movement using tSCS. Moreover, this is the first study to describe the benefits of tSCS in improving hand function in case of peripheral injury.
Methods
Participants
We performed transcutaneous stimulation of the cervical spinal cord in two individuals with tetraplegia resulting from C5 level motor complete spinal cord injuries and one individual with paralysis of the left hand due to peripheral nerve injury (median nerve at the wrist and suspected brachial plexus injury), but with an otherwise intact spinal cord. The details of the participants are summarized in Table 1. All procedures were approved by the Northwell Health Institutional Review Board. The study has been registered with ClinicalTrials.gov (NCT04755699).
Demographic and injury-related information for each participant.
Experimental sessions
Participants visited the lab for their sessions once per week. Their heart rate and blood pressure was measured at the beginning and end of each session. Electrodes were placed for recording bipolar EMG from the following muscles of the left arm and hand: biceps brachii (BIC), triceps brachii (TRI), flexor digitorum profundus (FDP), extensor digitorum communis (EDC) and abductor policis brevis (ABP). Force generated by the isometric flexion of the muscles of interest and EMG activity was simultaneously recorded at the start of the session. Since both the participants had no movement in their fingers, we focused on the volitional control of the tricep muscle for the participants with SCI. Meanwhile, as the participant with the brachial plexus injury (CTS01) had residual movement in the fingers of the left hand, we focused on the volitional control of the D1 interphalangeal (D1 IP) joint and lateral pinch. For evaluating the forces generated by the tricep muscle, the participants’ arms were extended out in front of them, with the hand in a neutral position and a load cell placed under the ulnar head prominence at the wrist. The elbow was resting on the table and prevented from lifting up during the task. For measuring the D1 IP and lateral pinch forces, a custom rig was used as shown in Figure 1. The experimenter cued the participants to push against the force sensor for 3-5 secs and then asked to relax for 3-5 secs. The task was performed in 2 sets of 5 trials each with a 60-90 secs of rest period between the sets. Verbal encouragement was provided to encourage the participants to generate maximal maintainable force.

A) Schematic showing the location of a 1 × 3 activated electrode configuration superimposed over the human spinal cord showing the dorsal column and roots. B) The custom electronically configurable electrode array placed over the cervical spinal cord of a study participant with a 1 × 3 configuration of activated electrodes (green LEDs). C) Setup for measuring tricep force. The ulnar protrusion of the wrist is placed over the 25 lb load cell during the task (red dashed square). D-E) Using the custom-built rig with a 10 lb load cell (gray puck) for measuring the force using D1 interphalangeal joint and lateral pinch, respectively in case of participant CTS01.
Transcutaneous spinal cord stimulation
Stimulation was provided using a custom-built stimulator and electrode array. The electrode array consisted of gold or silver-plated square contacts (10 mm x 10 mm) arranged in an 8 × 5 pattern with a 1 mm inter-electrode separation. To target specific cervical segments, an electrode configuration of 1 × 3 was used wherein 3 adjacent contacts within a single row, spanning the midline, were used. The electrode array was affixed to the back of the neck using a rectangular piece of proprietary hydrogel. To ensure consistency in placement of the array between sessions, we used the inion of the external occipital protuberance as a landmark. Distances measured from the inion were used to place the electrode array and identify the location of stimulation. Two 5 × 10 cm rectangular self-adhesive hydrogel electrodes (Axelgaard Manufacturing Co., Ltd., USA) placed along the midline over the lumbar spinal cord served as return electrodes.
Stimulation consisted of a 10 kHz multiphasic sinusoidal waveform that was 1 ms long for generating recruitment profiles. The waveform length was reduced to 0.5 ms during therapy to reduce neck muscle activation and increase participant comfort. The stimulation frequency was chosen to be 3 Hz for characterizing recruitment curves and 30 Hz during therapy.
EMG signal processing
We simultaneously recorded bipolar EMG from the following muscles of the left arm and hand: biceps brachii (BIC), triceps brachii (TRI), flexor digitorum profundus (FDP), extensor digitorum communis (EDC) and abductor policis brevis (ABP). We used pre-gelled Ag/AgCl electrodes, a differential amplifier (AD6221), and a signal digitizer (PicoScope® Model 4824A). The sampling rate used was 10 MHz while characterizing the recruitment profile of the upper limb muscles and 10-20 kHz during task performance. For characterizing the area-under-the curve (AUC), the EMG signal was filtered using a 60Hz IIR comb filter and Butterworth bandpass filter between 10-1000 Hz using a digital filter in MATLAB.
Recruitment profile
Stimulation consisted of a 1ms-long multiphasic pulse of the 10 kHz sinusoidal waveform at a stimulation frequency of 3 Hz delivered using an electronically-selected configuration of three contacts within a single row spanning the midline. Stimulation amplitudes tested ranged from 100 mA to up to 225 mA in intervals of approximately 25 mA. This was repeated for each of the eight rows of electrodes on the array. EMG was sampled at 10 MHz. The Picoscope 6 acquisition software was used to trigger acquisition of a 100 ms-long EMG signal following each stimulation pulse. For each stimulation amplitude and at each electrode row, we recorded such an EMG signal from 20-30 repetitions of the stimulation pulse. All the data was imported into MATLAB for further analysis. From each of the EMG signals recorded, we isolated a snippet starting from 5 ms and ending at 55ms after the stimulation artifact. We measured the peak-to-peak amplitude (P2P) for this snippet if the maximum amplitude of the snippet was greater than 5 times the standard deviation of baseline signal of that recording channel. For each muscle, the P2P amplitudes were normalized to the maximal P2P amplitude recorded across all amplitudes and electrode rows.
Results
Our results demonstrate that targeted transcutaneous spinal cord stimulation paired with minimal exercise training resulted in a substantial and sustained increase in muscle activity and strength in specific upper-limb muscles in two patients with motor complete cervical SCI and one participant with a peripheral injury. All three participants received stimulation for up to 1hr once per week. Blood pressure and heart rate monitoring at the start and end of each session showed no adverse effects of the stimulation.
Recruitment of upper limb muscles through targeted tSCS
We characterized the recruitment profile of the different motor pools innervating the upper limb muscles. To determine the effect of the location of stimulation along the rostro-caudal axis on the recruitment of the upper limb muscles, we sequentially delivered stimulation through the different rows of electrodes of the array (Figure 2A-C). Simultaneously, we recorded EMG activity from 5 muscles of the left arm and hand. Stimulation amplitude was increased and the corresponding increase in EMG amplitude was used as a measure of recruitment. We hypothesized that the recruitment pattern through transcutaneous stimulation would reflect the rostrocaudal segment-wise distribution of the upper limb motor nuclei in the cervical spinal cord. The recruitment profiles showed a distinct and consistent shape in all participants. Almost all the muscles exhibited the best recruitment when stimulation was delivered around the C5-C6 level. Stimulating using rostral electrodes primarily activated the biceps (Figure 2D, G and E, H), except in CTS03. Activation of the triceps invariably was strongest when stimulation was localized around the C5-C6 level. Stimulation using electrodes positioned more caudally resulted in decreased recruitment across all muscles. C8-T1 level stimulation showed recruitment of FDP and APB in participant CTS03 (Figure 2C, F and I). In participant CTS01, APB showed only weak recruitment irrespective of the location of stimulation, possibly due to the suspected brachial plexus injury. The fact that two participants had a spinal cord injury and metallic implants in the cervical vertebrae did not result in an obvious difference in the recruitment profile of the upper-limb motor pools is noteworthy. Additionally, we also determined the threshold of activation for each of the upper limb muscles. The thresholds of activation showed similar results as the recruitment profiles with biceps and/or triceps muscles having a low threshold of activation during rostral stimulation.
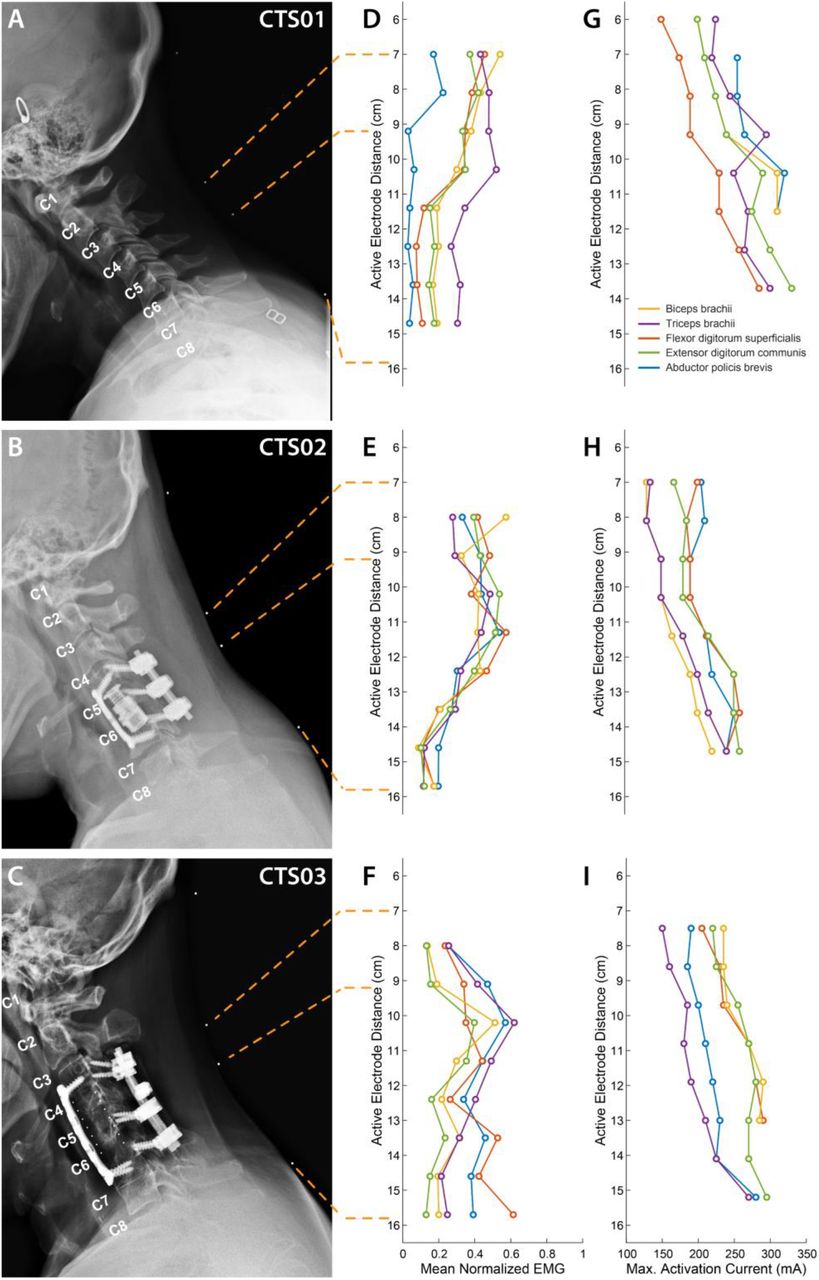
A-C) X-ray images in the sagittal plane with radio-opaque markers on the neck (white dots) for the three participants. The topmost marker identifies the inion of the external occipital protuberance. The second and third markers identify points 7 cm and 9.2 cm respectively, from the inion signifying the first and third rows of a putative electrode array whose first row of electrodes was aligned at 7cm from the inion. The last marker identifies the location of the last row of the putative electrode array at 15.7 cm from the inion. The cervical labels mark the exit point of the respective dorsal roots. D-F) Mean activation of the 5 muscles across all stimulation amplitudes mediated by tSCS through each of the 8 electrode rows. G-I) Stimulation amplitude that resulted in maximal activation of each of the 5 muscles.
Increased muscle activity and force generated with tSCS
To study the effect of tSCS on muscle force and activity, we asked the participants to perform specific activities using custom-made rigs. The rigs were designed to measure the force generated during the activity. We focused on specific muscles for each of the participants. For the participant with the brachial plexus injury, we focused on the muscles of the thumb. We observed a 715% increase in the force generated during the flexion of D1 IP joint (Figure 3A). This was accompanied by an increase in EMG activity of the left APB muscle (Figure 3B). We did not observe any major increase in the lateral pinch force during this period. For participants CTS02 and CTS03, we observed an increase of up to 1295% and 1118%, respectively, in the force generated by the left tricep muscle (Figure 3C). We also observed a corresponding increase in EMG activity for the tricep muscle (Figure 3D).
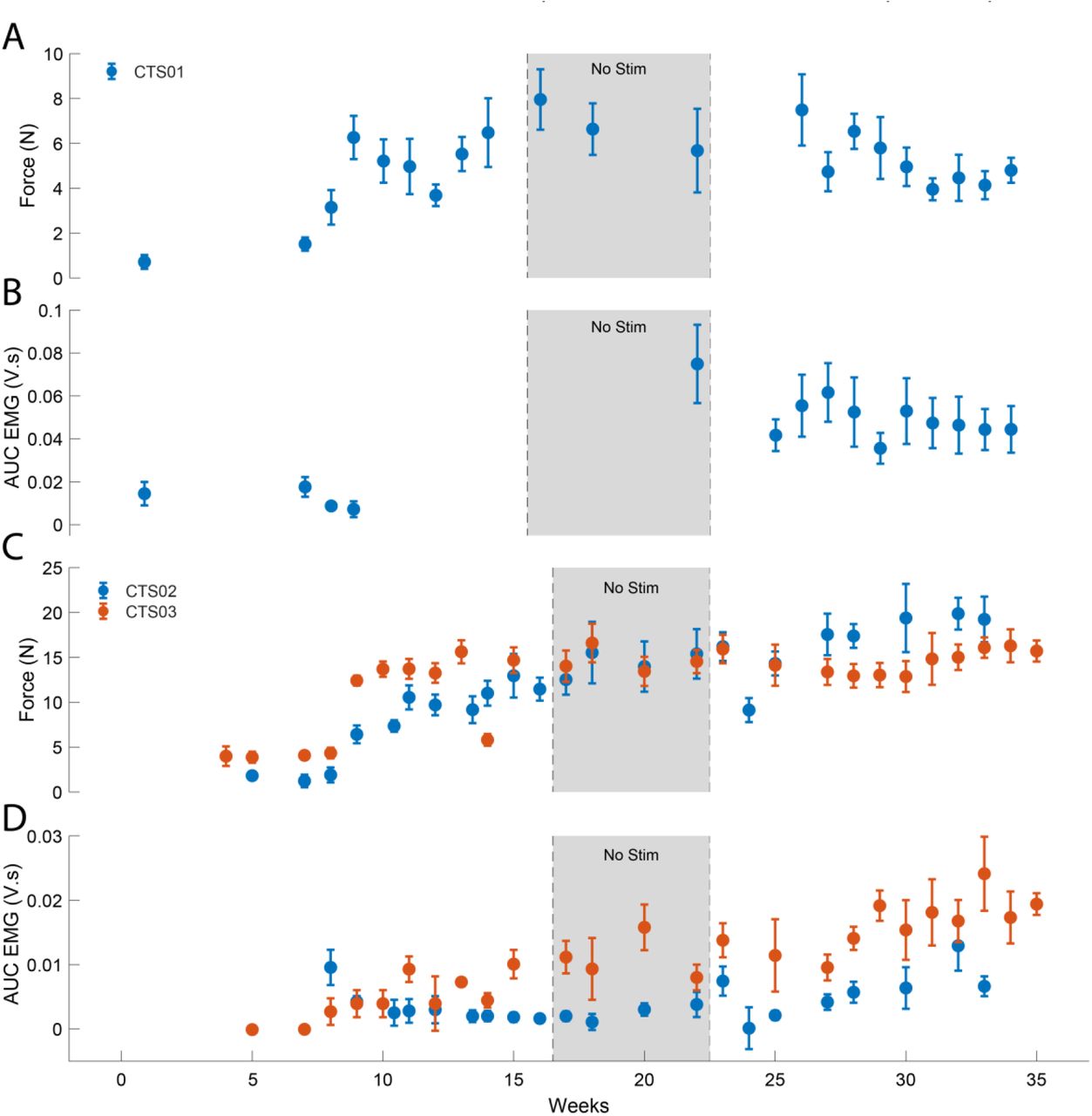
A) The force generated by the left D1 IP joint in case of participant CTS01. B) The AUC of the EMG activity recorded from the left APB muscle during the task of mforce generation using the D1 IP joint. C) The force generated by the left tricep muscle in case of participant CTS02 (blue) and CTS03 (orange). D) The AUC of the EMG activity recorded from the left tricep muscle during the task of force generation using the left tricep muscle.
GRASSP assessments
To evaluate the clinical significance of the progress showed by each participant, we also performed standard clinical assessments, namely the GRASSP test. GRASSP strength test showed only minor increases in the movements assessed, especially in the participants with SCI including the tricep muscle which was specifically targeted in this study (Figure 4A). GRASSP sensibility test showed decreases in sensation threshold at many locations in the hand in all participants (Figure 4B). For the participant with the brachial plexus injury, most of the improvement was observed in the thumb as well as the ulnar side of the hand. GRASSP strength showed increases in D1 IP and D5 abduction movements (Figure 4A). GRASSP sensibility showed up to a 3-point increase in sensation at the pinky tip (Figure 4B).

A) GRASSP strength change from baseline B) GRASSP sensibility change from baseline. Circles show 1- to 3-point increase in sensory perception as defined by the GRASSP sensibility scale. C) GRASSP prehension change in nut threading task for CTS01.
The nut threading task included in the GRASSP prehension tests showed an improvement in performing the right grasp (Figure 5A) and also a decrease in the time taken to perform the task (Figure 5B). Participants also shared their anecdotal descriptions of the effect of receiving tSCS. These mainly described increased control in moving their arms and being able to give “stronger hugs.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A) Snapshots showing improvement in grasping behavior from before tSCS therapy (first row) and week 42 of therapy (second row). B) Scatter plot shows the improvement in the time required to perform the task.
Discussion
In this study, we observed a substantial increase in volitionally generated force and EMG activity in specific muscles after paralysis from SCS in two individuals and peripheral injury in another individual (suspected brachial plexus injury). All three participants showed these changes within a short period of receiving tSCS. Interestingly, the improvements were restricted to the muscles that showed at least some measurable amount of force at the beginning of therapy. For instance, neither of the participants with SCI registered any force during finger flexion. We did not observe any improvement in the forces and EMG activity generated during finger flexion in either participant with SCI even when the activity was performed over many weeks while receiving tSCS. This could be due to tSCS not being targeted to the cervical levels that would have activated flexor motoneuron pools.
Our results are comparable to those demonstrated by other studies involving cervical tSCS in people with SCI (Inanici et al., 2021). However, our design involved minimal physical therapy and consisted of only one, 1-2 h long session per week. Importantly, our stimulation was targeted to achieve maximal recruitment of the muscle group of interest. This suggests that targeted tSCS could improve the efficacy of spinal cord activation and achieve restoration of volitional control even with minimal physical therapy.
The electrode configuration we used in this study was a 1 × 3 configuration spanning the spinal cord midline. The effectiveness of such an electrode configuration in recruitment of specific motorneuron pools has been demonstrated in able-bodied individuals (Gerasimenko et al., 2015; Krenn et al., 2015). It is highly likely that this configuration resulted in the stimulation of the dorsal column fibers thereby activating motor nuclei in off-target cervical levels and thus, reducing specificity. Activation of the dorsal roots via lateralized stimulation could result in greater selectivity in the motoneuron pools being activated. However, an earlier study with lateralized stimulation showed an increase in side-specific activation and not across spinal levels (Calvert et al., 2019). Previous studies have explored the idea of targeting stimulation above and below the injury level with the aim of enhancing the activity of the descending inputs as well as local circuitry below the site of injury. With a high cervical location of SCI (C5) for the participants in this study, most of the stimulation was restricted to being targeted at or below the injury level. In fact, stimulation targeted at higher cervical levels was perceived as uncomfortable by the participants. This demonstrates that tSCS can be tailored to suit patient comfort, target only those cervical levels innervating the muscle of interest, and still result in significant motor improvements.
Furthermore, we used a custom electrode array that could be electronically configured. This allowed efficient mapping and can support dynamic spatial pattern switching. In future studies, this feature can be combined with brain-computer interfaces (BCIs) to switch spatial patterns based on information decoded from intracortical activity (Bouton et al., 2016). Such automated configuration of targeted tSCS based on user movement intentions could improve the usability of this technology by people with SCI while performing activities of daily living.
It was interesting to observe improvement in somatosensory perception in regions innervated by spinal roots from below the injury level in both participants with SCI. To our knowledge, this is the first study to document improvements in sensation in people with SCI or peripheral injury after receiving tSCS. Stimulating dorsal roots of the spinal cord has been demonstrated to relay somatotopically relevant sensory information (Chandrasekaran et al., 2020). Meanwhile, restoring somatosensation through intracortical stimulation has been repeatedly demonstrated in humans as well (Flesher et al., 2016; Chandrasekaran et al., 2021; Fifer et al., 2021). It would be interesting to explore the benefits on pairing intracortical stimulation and tSCS for the long-term rehabilitation of somatosensation in SCI.
We believe this is the first study that performed tSCS in case of a peripheral injury (Lopez and Sdrulla, 2021) with the aim of restoring volitional control of hand movement. The rapid and significant improvement observed in the hand function in this case signifies major implications for a broader range of conditions affecting the central and peripheral nervous systems, including traumatic injuries and stroke.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Funding
This study was funded through support provided by Feinstein Institutes for Medical Research at Northwell Health.
Author Contributions
SC, NAB and CEB designed the study. SC, NAB, RR and CEB performed the experiments and SC analyzed the data. PDS and SJH provided critical feedback and input. All authors contributed towards interpreting the results of the experiments. SC and CEB finished the initial draft of the manuscript and all authors provided critical review, edits and approval of the final manuscript.
Competing Interest Statement
CEB has financial interests in Sanguistat, LLC and Neuvotion, Inc. and multiple patents in the neurostimulation field. The remaining authors have no conflicting financial interests.
Acknowledgements
We would like to thank our participants for their extraordinary commitment to this study, their patience with the experiments, and the deep insights provided by them, the clinicians and researchers at Feinstein Institutes for Medical Research. We would like to extend our deepest gratitude to Dan Sciubba, MD, David Bonda, MD and Karen Black, MD at Northwell Health for helping arrange the imaging sessions.
References



