
Abstract
Background Health Care Workers (HCWs) have been playing crucial role in treating patient with COVID-19. They have a higher occupational risk of contracting the disease than the general population, and a greater chance of them transmitting the disease to vulnerable patients under their care. Given their scarcity and low COVID-19 vaccine acceptance in Africa, it is essential that HCWs are seroprotected and their exposure to COVID-19 minimized. This study was therefore designed to determine IgG antibody response to SARS-CoV-2 among HCWs in North Eastern, Tanzania.
Methodology This was a cross-sectional study carried out among 273 HCWs at Kilimanjaro Christian Medical Centre (KCMC), a tertiary, zonal referral hospital in Tanzania’s North Eastern region. Stratified sampling was used to select study participants. Data were obtained from each consenting participant using a validated questionnaire. Blood samples were collected for SARS-CoV-2 IgG antibodies quantification by using an indirect ELISA test. RedCap software was used to enter and manage data. Statistical analysis was done by using STATA statistical software version 15 and GraphPad Prism v 9.0. A p-value of < 0.05 was considered the cut-off for statistical significance.
Results Among 273 HCWS only 37.9 % reported to have received COVID-19 vaccine. Except for one person, all of the participants had SARS-CoV-2 IgG antibody concentrations that were positive, with 64.5% of them having strong seropositivity. Female gender, allied health professionals, active smoking, COVID-19 patient interactions, COVID-19 vaccination receptivity, and adherence to recommended hand hygiene were found to be significant predictors of variation of median SARS-CoV-2 antibody concentration. The usage of personal protective equipment, history of previously testing PCR positive for COVID-19, the number of COVID-19 patient exposure and age were found to cause no significant variation in median antibody concentration among participants.
Conclusions This study reports a high seroprevalence of SARS-CoV-2 antibodies among healthcare workers in Kilimanjaro Christian Medical Centre. This suggests that HCWs have significant exposure to SARS-CoV-2 despite the low rate of vaccination acceptance even among HCWs. We recommend a strengthened Infectious Prevention and Control (IPC) in hospitals through provision of technical leadership and coordination according to WHO guidelines. We also recommend continued conduction of seroprevalence studies to estimate the magnitude and trends of SARS-CoV-2 infections in different populations in Tanzania. A better understanding of the past, current, and future transmission patterns of infectious pathogens is critical for preparedness and response planning, and to inform the optimal implementation of existing and novel interventions under the current and changing climate.
Introduction
The novel corona virus disease 2019 (COVID-19), is caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)(1,2). COVID-19 has been a large-scale global threat since 2019 with high global morbidity and mortality rates associated with economic disabilities, and social disruptions (3–5). WHO had reported a total of 115,500 deaths of HCWs in the world due to COVID-19 based on population estimates (6). COVID-19 is affects primarily the respiratory system with potential effects in other body organs (1,7). In Tanzania, the first case of COVID-19 was reported in 2020 indicating the virus global spread and its impact (8). Health care personnel have been on the front lines in taking care of COVID-19 patients, thus exposed to a higher occupational risk of contracting the disease than the general population. To protect this vulnerable group, WHO had implemented several initiatives, including making COVID-19 vaccination a priority for HCWs. Nevertheless, there has been a considerably low COVID-19 vaccine acceptance in Africa due to concerns regarding safety and efficacy issues, and associated side effects of the vaccines(9).
Immune responses to SARS-CoV-2 are directed to the four main structural proteins of the virus which are Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N) proteins (10). A specific humoral immune response against N and S protein has been reported and tend to persist in individuals (11,12). Immune responses to these proteins could be a result of either natural immunity from infection or vaccination (13). However, It has been also been reported that presence of neutralizing antibodies against these proteins correlates with the protection against future SARS-CoV-2 infection (14–16).
There is limited information regarding SARS-Cov-2 immunity among HCWS in Africa. Since antibody response is an acceptable proxy indicator of exposure to an infectious agent, (17), monitoring SARS-CoV-2 antibody response provides important information regarding the burden of exposure to SARS-CoV-2 among the higher risk group of HCWs is important. A better understanding of the past, current, and future transmission patterns of infectious pathogens including emerging and re-emerging infections is critical for preparedness and response planning, and to inform the optimal implementation of existing and novel interventions under the current and changing climate. The current study was designed to assess the seroprevalence of SARS-CoV-2 IgG antibodies among HCWs with different demographics in North-Eastern, Tanzania.
METHODOLOGY
Study setting and design
This was a cross sectional study, conducted from September to November, 2022. It was conducted in Kilimanjaro Christian Medical Centre, one of the four tertiary, zonal referral hospitals in Tanzania. It was purposively selected not only because it was a designed national center for managing COVID-19 cases during the pandemic but also its location in North-Eastern region of Tanzania. Kilimanjaro and Arusha are known for being the safari capitals of Tanzania, and popular stopovers for adventurers who are preparing for a Kilimanjaro trek. This makes Kilimanjaro region a vulnerable to cross border transmission of infectious diseases including SARS-CoV-2.
Study population
This study involved health care workers (HCWs) working at KCMC during the study period. Any person employed or volunteering in this setting was selected based on the definition of a HCW by WHO (18). If the selected HCWs did not consent to participate or donate a blood sample, then they were considered as ineligible for the study and thus excluded.
Sample Size and Sampling Technique
As there was no prior data on the prevalence of SARS-COV-2 antibodies among HCWs during the design of the study and in order to have sufficient sample size, an estimate of 50% as seroprevalence of SARS COV-2 antibodies among HCWs in Tanzania was considered. Using the formula by (19) and a desired precision of 0.05, and a confidence level of 0.95, a minimum sample size of 257 participants were required. However, to increase the power of analysis, 273 subjects were recruited in this study. To ensure fair healthcare workers’ representation, the population of healthcare workers in KCMC hospital was divided into 13 strata. These strata were represented by different hospital departments. Both inpatient and outpatient healthcare workers were selected from each stratum. Given the busy schedules and responsibilities of these healthcare workers, it was difficult to recruit them systematically for the study in their strata; therefore, a convenience sample of no more than 38 healthcare employees from each stratum was selected.
Data Collection procedures
Healthcare workers who consented to participate in this study were interviewed by using the study questionnaire embedded in Redcap Software installed on an Android tablet. This was a validated tool by WHO Regional Office for Africa (AFRO) to be used for healthcare workers (20) . Because it was a guidance for SARS-COV-2 antibody screening among HCWs for cohort studies, only questions used for participant enrollment were asked in this study. This adapted questionnaire included socio demographic and clinical characteristics, information about COVID-19 vaccination history, and COVID-19 illness, occupation and community-related behaviour during the pandemic.
Sample Collection
From each study participant a total of 2 mls of blood sample through vein puncture were collected under aseptic condition. Samples were stored in a cooler box (maintained at 4-8°C) in the field for a maximum of 3 hours before these samples get transferred to the Biotechnology Laboratory at Kilimanjaro Christian Research Institute for serum extraction. The samples that were collected had instantly their serum extracted upon arrival at Biotechnology Laboratory at Kilimanjaro Christian Research Institute. For serum extraction, samples were allowed to clot then they were centrifuged at 1000 g for 15 minutes. After that, the serum was collected and kept frozen at negative 20°C.
Detection of SARS-COV-2 Antibodies
IgG antibodies against SARS-CoV-2 were detected by using Generic Assays (GA) Enzyme-Linked Immuno-Sorbent assay (ELISA) for SARS-CoV-2 IgG Screening kits (MedipanGmbHGA Generic Assays GmbH, Ludwig-Erhard-Ring 3, 15827 Blankenfelde-Mahlow OT Dahlewitz, Germany). This indirect ELISA kit was a two-stage that focuses on the Spike and Nucleocapsid antigen of the SARS-CoV-2 virus detection. .The reported sensitivity and specificity of these GA ELISA tests are > 98% (21).
Statistical analysis
STATA statistical software version 15 was used to do all statistical tests. Hence, all data from the created spreadsheet was imported to STATA. Descriptive statistics were employed to summarize the study participant’s baseline socio-demographic, clinical, COVID-19 exposure history as well as the seroprevalence of antibodies against SARS-CoV-2. After verifying that SARS-CoV-2 IgG concentration among HCWs is not normally distributed (p =0.00132 by Shapiro Wilk test), non-parametric tests were performed to compare the significant difference between the exposure variables and median SARS-CoV-2 IgG concentration. The Mann–Whitney test was used for the comparison of antibody concentrations of two independent groups. The Kruskal–Wallis test was used for the comparison of more than two groups. A p-value of 0.05 was regarded as significant for the found associations
Ethical Considerations
Ethical clearance to carry out this study was obtained from the College Research Ethical Committee (CREC) of Kilimanjaro Christian Medical University College (KCMUCo), ethical clearance number PG61/2022. Permission from the participant hospital administration was sought after the proposal was submitted and accepted by the ethical committee. To conceal participants’ identities, the questionnaire and blood samples were labelled using numbers and letters.
RESULTS
Response rate
A total of 273 of the 279 participants in this study had results on their serum SARS-CoV-2 IgG concentration, resulting in a rate of response of 97.8%.
Demographic and Clinical-exposure Characteristics of the Study Participants
Among the 273 participants, half of the participants were under 32 years old, with a median age of 32 (IQR: 26-44) and a male predominance of 60.4% among the total number of participants. The majority of study participants were nurses (40.5 %) and had a normal BMI (41.3%). Less than half of the study participants received the COVID-19 vaccine, and only 8.8% reported being tested PCR positive for COVID-19 in the past. The vast majority of participants (94.1%) stated that they had never smoked, Table 1.
Occupation and Community Related Behaviour Factors during the Pandemic
Only 38.5% of the study participants wore mask at indoor setting outside their homes. A large proportion of participants (56.6%) practice good hand hygiene always as recommended, 38.9% follow IPC standard precautions when in contact with any patients, and fewer than half (42.4%) always wear PPE according to the risk assessment. Half of the study participant lived in a household size of 3-5 people and 39.5% used public transportation more than nine times a day, Table 2.
Seroprevalence of SARS-CoV-2 IgG Antibody Concentration among the Study Participants
Except for one person, all of the participants showed SARS-CoV-2 IgG antibody concentrations that were positive, with 64.5% of them having strong seropositivity, Figure 1. While comparing people who had received the COVID-19 vaccine and those who hadn’t, it was shown that the majority of the vaccinated individuals had strong seropositivity, Figures 2 and 3.



Socio-Demographic, Clinical, and Behavioural Characteristics Associated with Variation in Median SARS-CoV-2 IgG Concentration among Study Participants
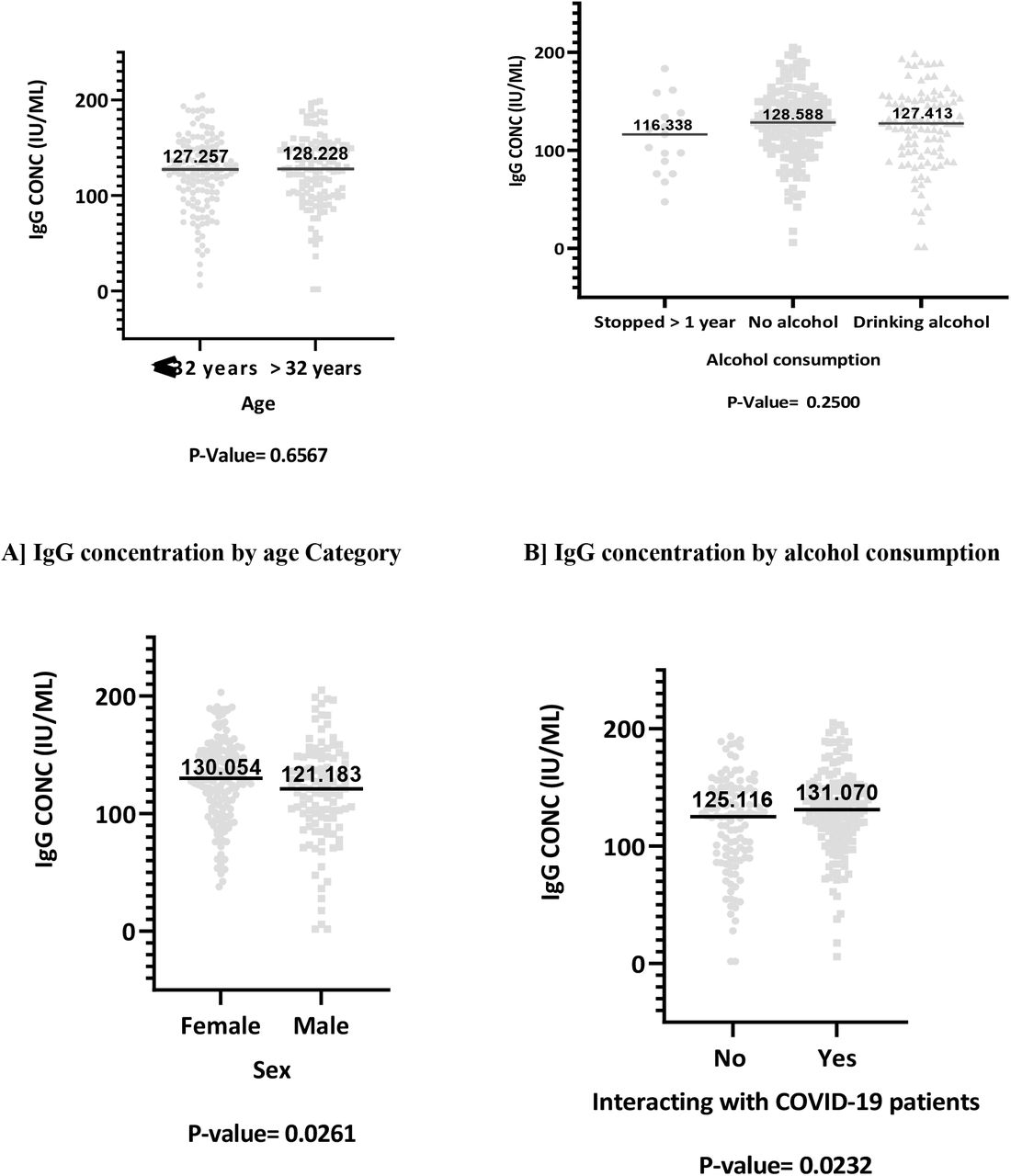
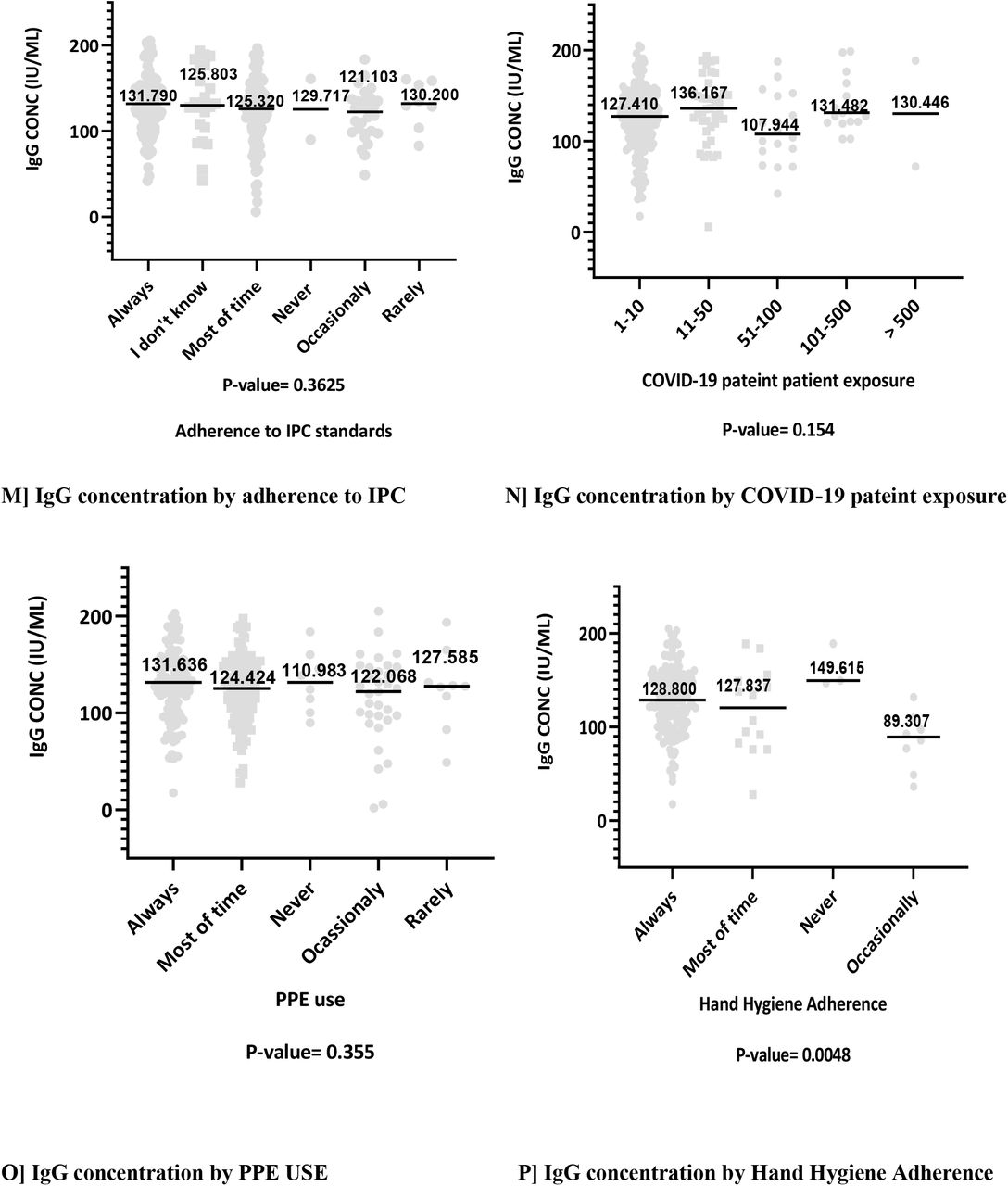
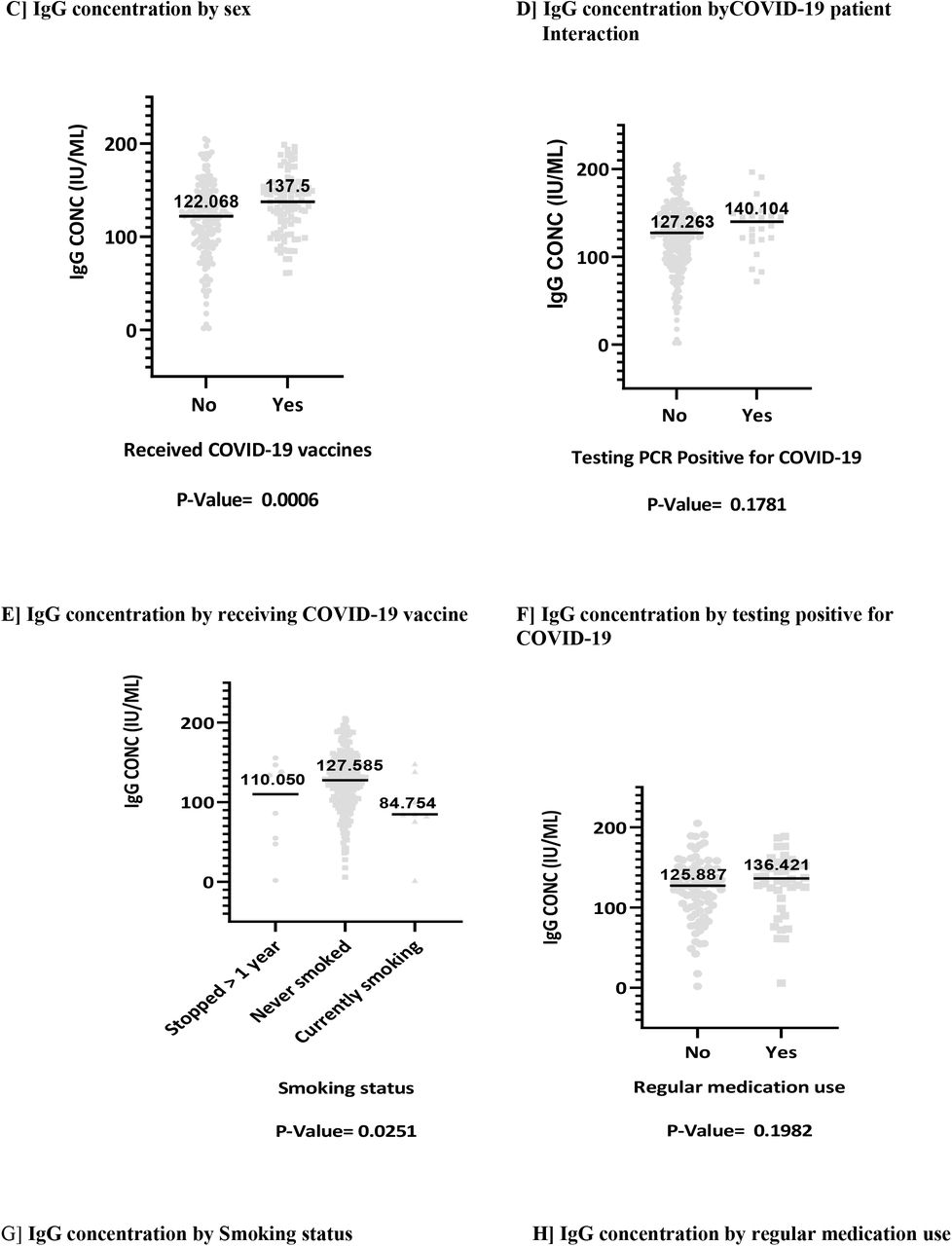
Sex, BMI, smoking status, adherence to recommended hand hygiene, cadre, and interaction with COVID-19 patients are variables that were found to significantly affect the median IgG concentration. IgG median concentration was significantly higher in females compared to males. It was found that those with obesity had significantly greater median concentrations than individuals with other BMI categories. Those who had never smoked had significantly higher SARS-CoV-2 IgG median concentrations than current smokers. Individuals, who followed recommended hand hygiene were found to significantly have a higher median concentration. Moreover, median concentrations were significantly greater in who interacted with COVID-19 patients. Interestingly, allied health proffessionals were found to have a significantly higher median concentration comparing to other health care workers. Other factors were assessed but found to not significantly causing differences in median SARSCOV 2 IgG concentration among participants, Figure 4.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This study aimed at determining the IgG antibody response to SARS-CoV-2 among HCWs in our institution. The finding revealed a remarkably seroprevalence of 99.6% among the sampled HCWs. Females, allied health professionals, obese people, HCWs who adhered to recommended hand hygiene practices, and those who interacted with COVID-19 patients more frequently had significantly higher median SARS-CoV-2 antibody concentrations. Other factors that were assessed did not reveal any significant variation in Median SARS-CoV-2 IgG concentration.
This higher seroprevalence of SARS-CoV-2 antibodies among HCWs indicates the high level of virus exposure in this population, and an existed risk of infection within the hospital. These results are also consistent with other studies that revealed high seroprevalence of SARS-CoV-2 antibodies among HCWs (22,23). However, this seroprevalence is higher than that reported in other East African countries (24–26). The level of COVID-19 pandemic precautions that was initially put in our country can explain this huge discrepancy with other East African countries.
Contrary to the expectation, this study did not find any significant difference in antibody concentration between healthcare workers considering their previous history of testing PCR positive for COVID-19. This is contradicting finding to other previous studies that indicated that previous SARS-CoV-2 infection leads to higher SARS-CoV-2 IgG antibodies concentrations (27–30). Several factors may have influenced these results. It might be due to the low percentage of healthcare workers who tested positive in this study. Also, the significant decline of SARS-CoV-2 antibody levels after infection may additionally explain this results (31). Hence, a time interval for antibody monitoring should be found so as to determine how long SARS-CoV-2 antibodies does lasts.
Regarding various cadres, this study found that allied health professional had a higher SARS-CoV-2 median concentration compared to other HCWs. This indicate that there was an increased risk of SARS-CoV-2 exposure among allied HCWS compared medical doctors and nursing cadres. Results are concordant with one previous observational study, which had shown increasing odds off seropositivity in allied health professionals compared to medical doctors (32). The reasons behind this finding are necessary to be explored in order to protect these allied HCWs from the risk of acquiring communicable diseases in their work setting
Another important finding was a higher median antibody concentration among healthcare workers who adhere to recommended hand hygiene during the pandemic. The finding of our study does not support other studies that found no association between self-reported adherence to hand hygiene and SARS-CoV-2 antibody positivity among HCWs (33). Hand hygiene is an important element of infection prevention practices in the hospital and reflects behavior, attitudes and beliefs (34). It may be hypothesized that HCWs who adhered to recommended hand hygiene were also more likely to receive COVID-19 vaccine. However, this hypothesis was not explored in this study.
Study finding has revealed that HCWs who interacted with COVID-19 patient had significantly higher median concentration. It is important to note that the number of COVID-19 patient the HCW is exposed to, does not predict seroconversion as per our study findings. Therefore, it confirms that COVID-19 patient exposure only is a significant factor for detecting SARS-CoV-2 antibodies among HCWs. These results match those observed in earlier studies that demonstrated that regular interaction with COVID-19 patients increases one’s risk of contracting SARS-CoV-2 (27,35–39). It can be hypothesized that relying solely in number of COVID-19 patient in hospitals led to inadequate HCWs protection.
According to our findings, females had higher median concentrations of SARS-CoV-2 antibodies than males. This supports the theory that after disease exposure, females have higher antibody production compared to males because male androgens suppress the immune response (40). Contrary to our findings, several other studies have found that male HCWs have higher SARS-CoV-2 antibodies than female HCWs, inferring to behavioural differences (25,27,37,41,42). During the pandemic, male had a worse clinical outcomes and mortality (Kopel et al., 2020; O’Brien, Du and Peng, 2020). The argument can be that the immune response of female played a major role in Clinical outcome of COVID-19 rather than behavioural differences with males.
The findings from this study indicate that individuals who currently smoke had a lower antibody response to SARS-CoV-2. This may be due to the fact that smoking increases the clearance of circulating antibodies by enhancing the production of monocytes and macrophages (43). It can also can be evidenced by the reduction of antibody titers after COVID-19 vaccination in individuals who smoke (44). However, some other studies have found no association between smoking and SARS-CoV-2 antibody concentrations (45,46). The study methodology and demographic characteristics between studies may explain this finding variations between studies.
5.1 Conclusion
This study has revealed a high prevalence of SARS-CoV-2 IgG antibodies among HCWs in our setting. These results reveal that most HCWs are exposed to SARS-CoV-2 infection and thus probably more seroprotected.
5.2 Study limitations and strengths of the study
This study has successfully demonstrated its purpose, but the scope of this study was limited as such, retrospective assessment of self-reported exposures may be subject to recall bias. This study was conducted in one centre, a tertiary hospital where exposure to the SARS-CoV-2 virus cannot be underestimated. Therefore, a caution must be applied in a nationwide result generalization. Notwithstanding these limitations, this is the first study surveying the seroprevalence of SARS-CoV-2 IgG antibodies among healthcare workers in Tanzania.
5.3 Recommendation
This research has thrown up many questions in need of further investigation. More broadly, future research should focus in large cohort to determine the long-term implication of SARS-CoV-2 antibodies such as probability of reinfection and the outcome of vaccination uptake among HCWS in our setting. A reasonable approach tackle HCWs disease exposures is to implement strict preventive measures for communicable diseases in society to reduce the burden in hospitals.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Financial Disclosure statement
The East African Consortium of Clinical Research (EACCR) under EDTCP funds sponsored this study as a component of the large project “Emerging and Re-emerging Neglected Infectious Disease”.
Competing interests
None Declared
References




