
Abstract
Background Cancer is a serious threat to the whole of humanity. The Multi-Cancer Early Detection (MCED) test is expected to solve the problem of “Universal cancer screening”. The purpose of this study is to evaluate the screening performance of two MCED tests, YiDiXie™-HS and YiDiXie™-SS, in multiple cancer types.
Patients and methods 11094 subjects were finally included in this study (the malignant tumor group, n = 4405; the normal control group, n = 6689). The malignant tumor group included all solid and hematological malignant tumor types covered in “China cancer registry annual report” by the National Cancer Center of China. The sensitivity and specificity of YiDiXie™-HS and YiDiXie™-SS were evaluated, respectively.
Results The overall sensitivity of YiDiXie™-HS for different cancer types and stages was 90.1% (89.2% - 90.9%; 3971/4405), and its specificity was 89.7% (89.0% - 90.4%; 6002/6689). Its sensitivity increases with clinical stage: stage I, 85.6% (83.9% - 87.1%); stage II, 91.4% (89.6% - 93.0%); stage III, 93.9% (92.0% - 95.4%); and stage IV, 98.4% (96.9% - 99.2%). The overall sensitivity of YiDiXie™-SS for different cancer types and stages was 99.1% (98.8% - 99.3%; 4365/4405), and its specificity was 65.2% (64.0% - 66.3%; 4358/6689). Its sensitivity was basically comparable in each clinical stage: stage I, 98.6% (98.0% - 99.1%); stage II, 99.5% (98.9% - 99.8%); stage III, 99.5% (98.6% - 99.8%); stage IV, 99.8% (98.9% - 100.0%).
Conclusion YiDiXie™-HS has a high sensitivity in all clinical stages of all cancer types and can be a powerful complement to existing cancer screening tests. YiDiXie™-SS has an extremely high sensitivity in all clinical stages of all cancer types and is expected to solve the world problem of “Universal cancer screening”.
Clinical trial number ChiCTR2200066840.
INTRODUCTION
The World Health Organization’s International Agency for Research on Cancer (IARC) released data on the global cancer burden in 2020, showing that in 2020, there were 19.29 million new cancer cases and 9.95 million cancer deaths globally; there were 4.57 million new cancer cases and 3 million cancer deaths in China, with the number of new cancer cases and deaths ranking first in the world1. Therefore, cancer is a serious threat to Chinese and the whole of humanity.
Cancer imposes a heavy financial burden on society, with total cancer treatment expenditures in the United States alone exceeding $200 billion in 20202-4, and projected to reach $246 billion in 20305. In addition, cancer treatment imposes a significant financial burden on patients, with patient out-of-pocket expenditures for cancer treatment in the United States estimated at $16 billion annually6; 12% to 62% of cancer patients in the United States are reported being in debt because of their treatment7. Thus, cancer places a heavy financial burden on society and patients.
“Universal cancer screening” can significantly improve patient prognosis8-14, dramatically reduces socio-economic burdens15-17, markedly improves patients’ economic status6,16,18 and significantly improve patient employment19.
However, the screening model of existing cancer screening tests does not fulfill the need for “Universal cancer screening”. This screening model20 can be referred to as the model of “Single-Cancer Early Detection (SCED)”, which refers to the application of existing cancer screening tests (e.g., CT, ultrasound, gastroscopy, colonoscopy, blood TPSA, etc.) to screen for one site-specific cancer at a time (e.g., CT scan for lung cancer, mammogram for breast cancer, TPSA for blood, etc.), and Subjects undergo multiple examinations or tests to screen for multiple cancers.
Several shortcomings of the SCED model limit its use in “Universal cancer screening”. First, the public often forgoes cancer screening due to concerns that the screening process is too cumbersome16, the tests are expensive21, and some of the tests are invasive and radioactive21-25. Second, the SCED model does not enable “Universal cancer screening” due to the low incidence of the individual cancer types screened. Conventional guidelines recommend “high-incidence cancer screening for high-risk populations” not “universal cancer screening”26-30, which consequently leads to a poorer prognosis for the majority of cancer cases 8,9,12,31. Finally, the SCED model leads to a large accumulation of false-positive results32 and significantly increases patient anxiety33,34 and subsequent medical costs32,35. Therefore, there is an urgent need to find a better screening model to fulfill the need of “Universal cancer screening”.
Recently, a new blood test called the “Multi-Cancer Early Detection (MCED) test” or “Pan-cancer test” has been developed, which allows for the early detection of multiple cancers with a single blood test 36-38. They typically combine artificial intelligence (AI) and machine learning with the detection of a variety of circulating analytes, including free cell DNA (cfDNA), circulating tumor cells (CTCs), miRNAs, exosomes, and others, to detect early signs of multiple cancers37-39. These MCED tests have generated a new model of cancer screening, the MCED model, and is expected to solve the world’s problem of “Universal cancer screening”.
Based on the detection of miRNAs in serum, Shenzhen KeRuiDa Health Technology Co., Ltd. has developed “YiDiXie™ all-cancer test” (hereinafter referred to as the “YiDiXie™ test”). With only 200 milliliters of whole blood or 100 milliliters of serum, the test can detect multiple cancer types, enabling early detection of cancer at home. The “YiDiXie™ test” consists of three independent tests: YiDiXie™-HS, YiDiXie™-SS and YiDiXie™-D.
The purpose of this study is to evaluate the screening performance of two MCED tests, YiDiXie™-HS and YiDiXie™-SS in multiple cancer types.
PATIENTS AND METHODS
Study design
The SZ-PILOT study (ChiCTR2200066840) was a single-center, prospective, observational study. Subjects who signed the broad informed consent for donation of remaining samples at the time of admission or medical health checkup were included, and 0.5 ml of their remaining serum samples were collected for this study.
This study was blinded. Neither the laboratory personnel performing the “YiDiXie™ test” nor the technicians of KeRuiDa Co. evaluating the raw results of the “YiDiXie™ test” were informed of the subject’s clinical information. The clinical experts assessing the subjects’ clinical information were also unaware of the results of the “YiDiXie™ test”.
The study was approved by the Ethics Committee of Peking University Shenzhen Hospital and was conducted in accordance with the International Conference on Harmonization for “Good clinical practice guidelines” and the Declaration of Helsinki.
Participants
Subjects in the two groups were enrolled separately, and all subjects who met the inclusion criteria were included consecutively.
The malignant tumor group initially enrolled hospitalized patients with “suspected (solid or hematological) malignant tumors” with a signed broad informed consent for donation of the remaining samples. Subjects with tumor that has been surgically removed or disappeared after treatment at the time of sample acquisition, no surgical or biopsy pathology diagnosis, or ambiguous pathology were excluded from the malignant tumor group.
The normal control group initially included healthy medical examiners signing a broad informed consent for donation of the remaining samples. Subjects with undiagnosed suspected malignant tumors were excluded from the normal control group.
Subjects who were not qualified in the serum sample quality test prior to the “YiDiXie™ test” were excluded from the study.
Sample collection, processing
The serum samples used in this study were obtained from serum left over after a normal consultation, without the need for additional blood sampling. Approximately 0.5 ml of serum was collected from the remaining serum of the participants in the Medical Laboratory and stored at - 80°C for use in the subsequent “YiDiXie™ test”.
“YiDiXie™ test”
The “YiDiXie™ test” is performed using the “YiDiXie™ all-cancer detection kit”. The “YiDiXie™ all-cancer detection kit” is an in-vitro diagnostic kit developed and manufactured by Shenzhen KeRuiDa Health Technology Co., Ltd. for use in fluorescent quantitative PCR instruments. It detects the expression levels of dozens of miRNA biomarkers in serum to determine whether cancer is present in the subject. It predefines appropriate thresholds for each miRNA biomarker, ensuring that each miRNA marker has a high specificity (≥0.95). The YiDiXie™ kit integrates these independent assays in a concurrent testing model to significantly increase the sensitivity in broad-spectrum cancers and maintain a high specificity.
The “YiDiXie™ test” consists of three tests with highly different characteristics: YiDiXie™-HS, YiDiXie™-SS and YiDiXie™-D. The YiDiXie™-HS (YiDiXie™-Highly Sensitive) is the standard version of the “YiDiXie™ test”, which was developed with high sensitivity and high specificity. On the basis of YiDiXie™-HS, YiDiXie™-SS (YiDiXie™-Super Sensitive) significantly increases the number of miRNA tests to achieve extremely high sensitivity for all stages in all malignancy types. Based on YiDiXie™-HS, YiDiXie™-D (YiDiXie™-Diagnosis) significantly increases the diagnostic threshold of individual miRNA tests to achieve very high specificity. YiDiXie™-D is designed for preoperative diagnosis of a wide range of tumors, and therefore its early cancer screening performance was not evaluated in this study.
Perform the “YiDiXie™ test” according to the instructions of the “YiDiXie™ all-cancer detection kit”. Briefly, take 20 μl of serum, add 20 μl of Nucleic Acid Extract, mix well and centrifuge at 50 °C for 20 minutes, 95 °C for 5 minutes, and 13,000 rpm at 4 °C for 5 minutes, and the supernatant is the Nucleic Acid Extract. Take 8 μl of crude nucleic acid extract, add 12 μl of reverse transcription reaction solution, mix well, keep warm at 37 °C for 30 min, keep warm at 42 °C for 30 min, heat at 75 °C for 5 min, and leave on ice for 2 min. cDNA was diluted by 20-fold for further analysis. Take 4 μl of cDNA dilution solution, add 6 μl of amplification solution, mix well, and then carry out RT-qPCR reaction program. The RT-qPCR running program was set up as follows: 95 °C for 2 min, then 40 cycles of 95 °C for 10s, 60 °C for 30 s and 70 °C for 30s.
The original test results were analyzed by the laboratory technicians of KeRuiDa Co. and determined to be “positive” or “negative”.
Clinical data collection
Clinical, pathological, laboratory, and imaging data in this study were extracted from the subjects’ hospitalized medical records or physical examination reports. Clinical staging was completed by trained clinicians assessed according to the AJCC staging manual (seventh or eighth edition) 40,41.
Statistical analyses
For demographic and baseline characteristics, descriptive statistics were reported. For categorical variables, the number and percentage of participants in each category were calculated; for continuous variables, the total number of participants (n), mean, standard deviation (SD) or standard error (SE), median, first quartile (Q1), third quartile (Q3), minimum, and maximum values were calculated. The 95% confidence intervals (CIs) for multiple indicators were calculated using the Wilson (score) method.
RESULTS
Participant disposition
A total of 11754 study subjects (The malignant tumor group, n = 4963; The normal control group, n = 6791) were initially enrolled in this study (Fig. 1). 102 cases in the normal control group were excluded due to undiagnosed suspected tumors. A total of 558 cases were excluded from the malignant tumor group, of which 345 cases had no pathological results, 170 cases with tumors surgically removed or regressed after treatment, and 43 cases had ambiguous benign or malignant pathological results. There were no samples that failed the test due to substandard serum quality, which was mainly due to the fact that the samples used in this study were residual serum after regular test, substandard samples had been excluded by the medical laboratory, and the samples were stored under good conditions. Mild hemolysis or samples stored at unsuitable temperatures can lead to test failure. All exclusion categories were preset before enrollment. This study finally included 11094 study subjects (The malignant tumor group, n = 4405; The normal control group, n = 6689).

Subject enrollment in this study.
Table 1 lists the demographic and clinical characteristics of the 11094 participants. The two groups of participants were comparable in terms of demographic and clinical characteristics (Table 1). There was an expected difference in age group distribution between the malignant and normal groups (i.e., more cancers than non-cancers in the older age groups). The mean (standard deviation) age was 51.7 (13.44) years and 46.6% (5172/11094) were female (comparable proportions in both groups). 66.9% (2764/4405) of the malignant tumor group were stage I/II.
The malignant tumor group includes all types of malignant tumors covered in the “China cancer registry annual report” by the National Cancer Center of China (including all solid and hematological malignant tumors): oral cavity, pharynx, larynx, brain, nasopharynx, thyroid, lung, esophagus, stomach, colorectum, breast, liver, gallbladder, pancreas, kidney, urinary tract, ovary, uterus, cervix, prostate, testicle, penis, lymphoma, leukemia42. In this study, “others” refers to malignant tumor types other than those listed above, such as adrenal cancer, vulvar cancer, skin cancer, melanoma, metastatic cancer of unknown primary site, etc.
Performance of YiDiXie™-HS
The overall sensitivity of YiDiXie™-HS for different cancer types and stages was 90.1% (95% CI: 89.2% - 90.9%; 3971/4405) and the specificity was 89.7% (95% CI: 89.0% - 90.4%; 6002/6689) (Table 2).
The sensitivity of YiDiXie™-HS increased with increasing stage in different clinical stages: stage I, 85.6% (83.9% - 87.1%); stage II, 91.4% (89.6% - 93.0%); stage III, 93.9% (92.0% - 95.4%); stage IV, 98.4% (96.9% - 99.2%) (Table 3). Therefore, YiDiXie™-HS has high sensitivity for all clinical stages.
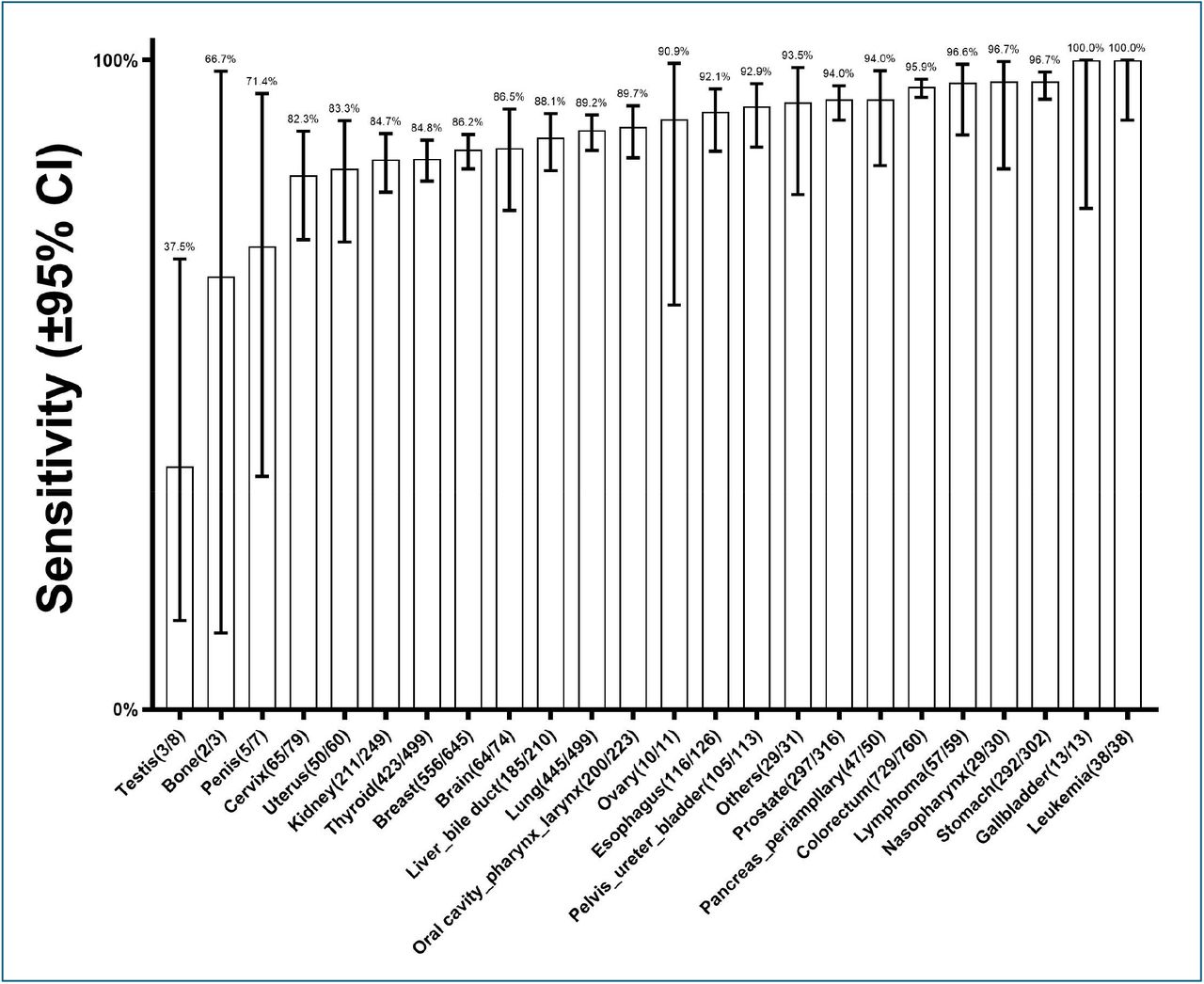
The sensitivity of YiDiXie™-HS for different malignant tumor types is shown in Figure 2. The sensitivity of the most of the malignant tumor types range from 82.3% to 96.7%, except for a few cancer types with a small number of cases. Therefore, YiDiXie™-HS has high sensitivity for all cancer types.
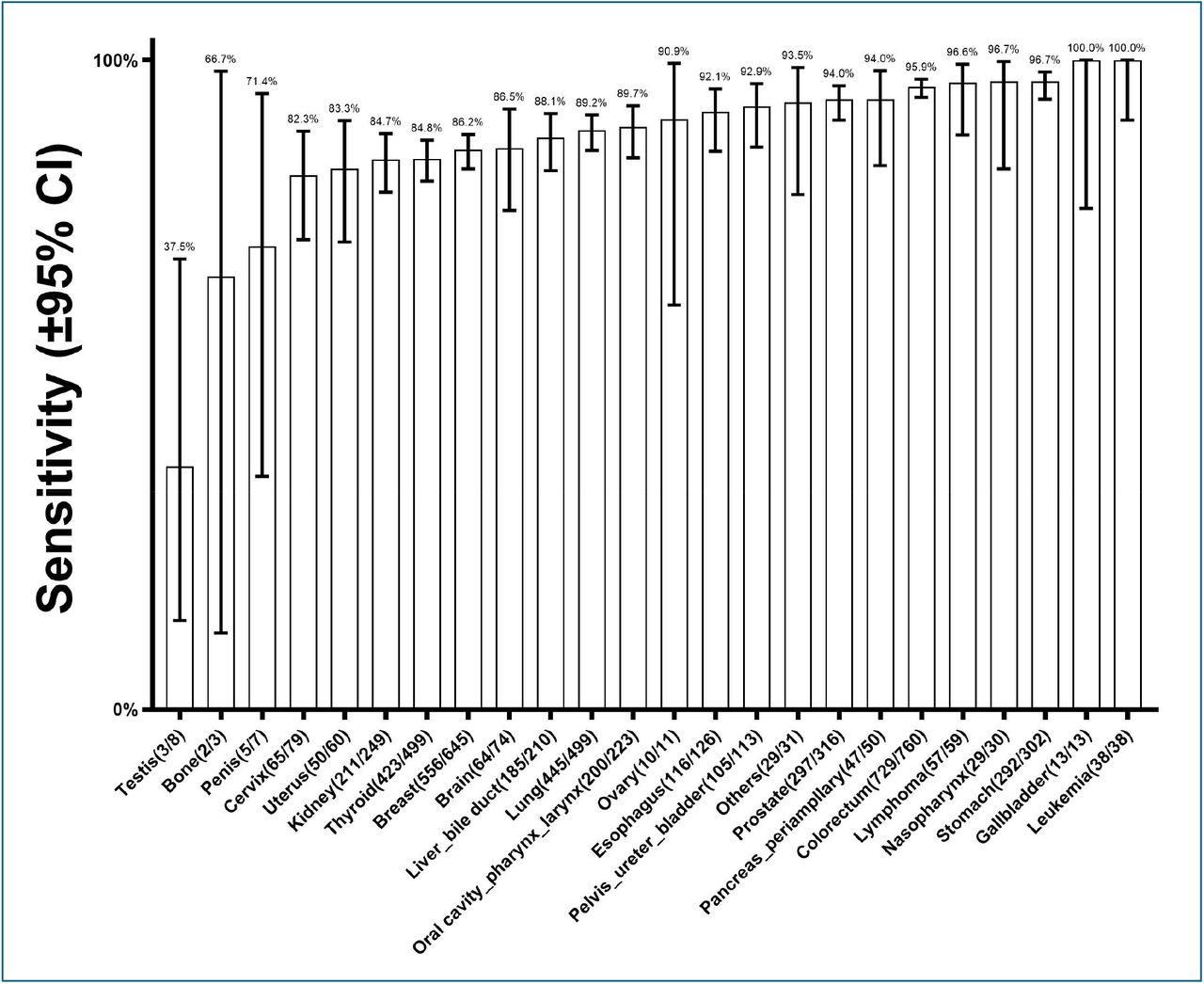
Sensitivity of YiDiXie -HS in different malignant tumor types. The horizontal axis shows different malignant tumor types, including all malignant tumor types (including all solid and hematological malignant tumors) covered in “China cancer registry annual report” by the National Cancer Center of China. “Others” are malignant tumor types other than those mentioned above. Bars represent 95% confidence intervals.
Figure 3 reports the sensitivity of YiDiXie™-HS for 16 cancer types with clinical stages and a large number of cases. The results show that YiDiXie™-HS has high sensitivity for all stages of these 16 cancer types, except for a few clinical stages with few cases.
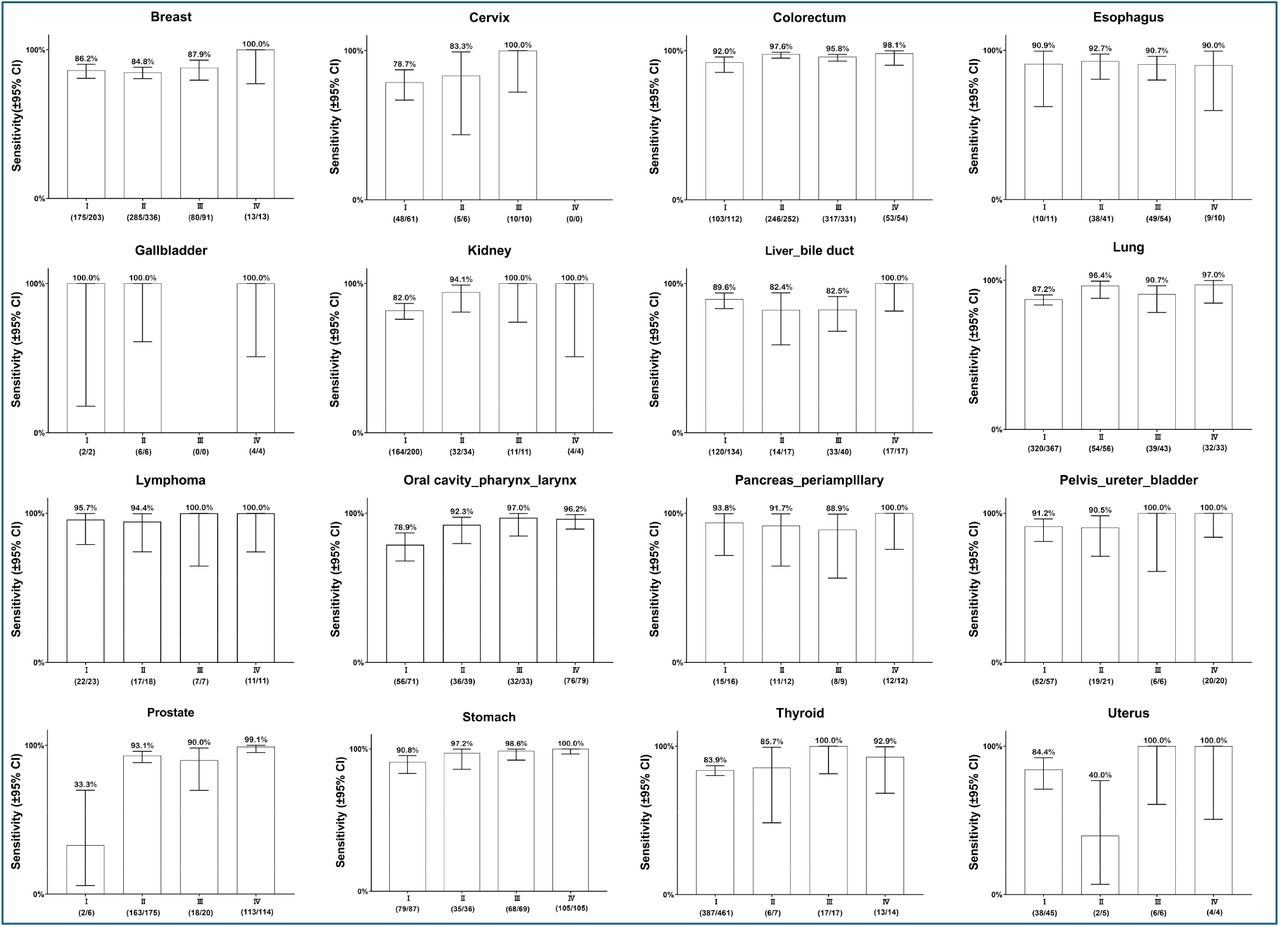
Sensitivity of YiDiXie -HS in 16 cancer categories with a high number of clinically staged cases. Bars represent 95% confidence intervals.
Performance of YiDiXie™-SS
The overall sensitivity of YiDiXie™-SS for different cancer types and stages was 99.1% (95% CI: 98.8% - 99.3%; 4365/4405) and its specificity was 65.2% (95% CI: 64.0% - 66.3%; 4358/6689) (Table 4).
The sensitivity of YiDiXie™-SS was equivalent across clinical stages: stage I, 98.6% (98.0% - 99.1%); stage II, 99.5% (98.9% - 99.8%); stage III, 99.5% (98.6% - 99.8%); stage IV, 99.8% (98.9% - 99.8%) (Table 5). Therefore, YiDiXie™-SS has a very high sensitivity for all clinical stages.
The sensitivity of YiDiXie™-SS for different malignant tumor types is shown in Figure 4. The results showed that the sensitivity for various cancer types ranged from 97.3% to 100%. Therefore, YiDiXie™-SS has very high sensitivity in all cancer types.
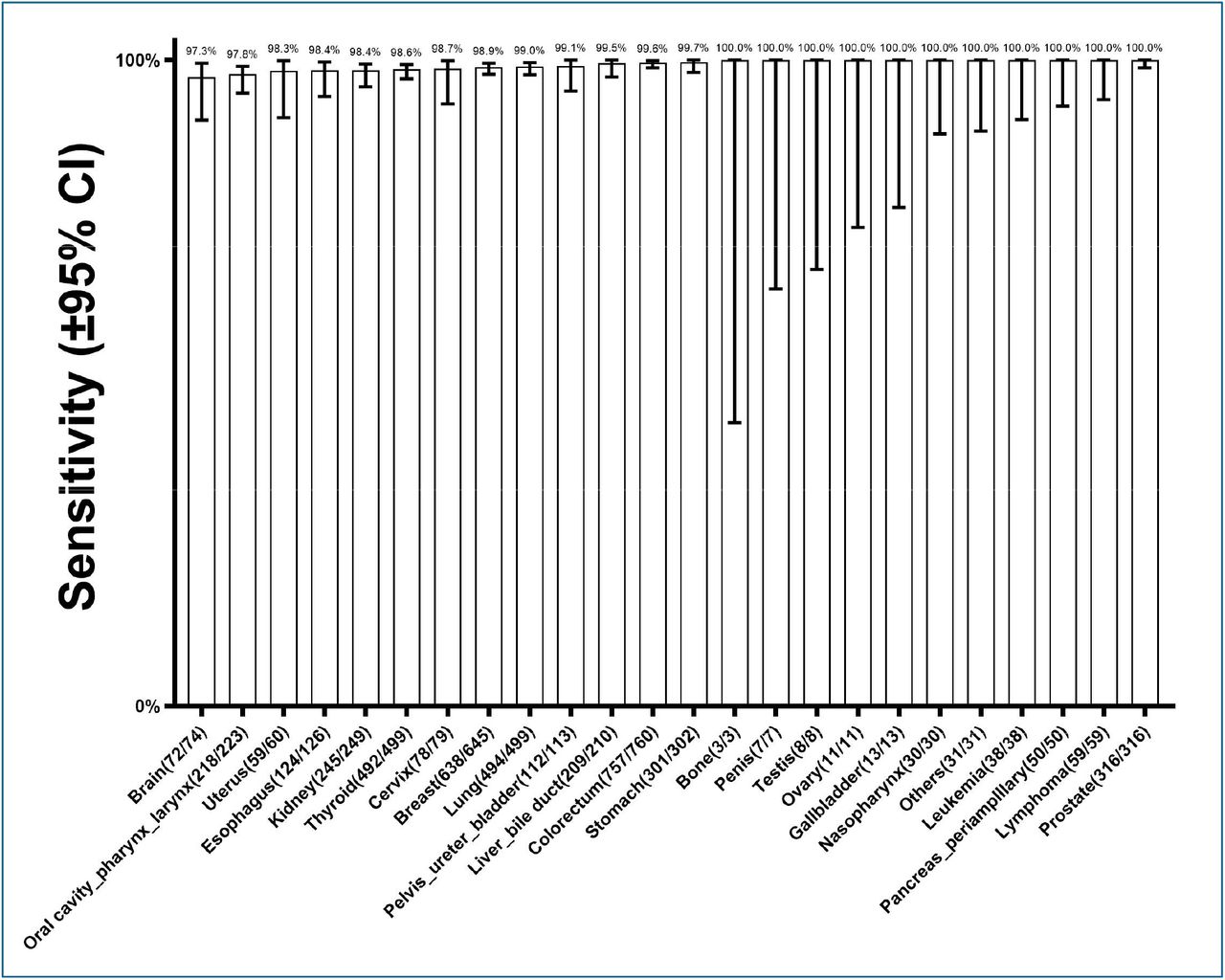
Sensitivity of YiDiXie -SS in different malignant tumor types. The horizontal axis shows different malignant tumor types, including all malignant tumor types (including all solid and hematological malignant tumors) covered in “China cancer registry annual report” by the National Cancer Center of China. “Others” are malignant tumor types other than those mentioned above. Bars represent 95% confidence intervals.
Figure 5 reports the sensitivity of YiDiXie™-SS for 16 cancer types with clinical stages and a large number of cases. The results show that YiDiXie™-SS has very high sensitivity in all stages of these 16 cancers.

Sensitivity of YiDiXie -SS in 16 cancer categories with a high number of clinically staged cases. Bars represent 95% confidence intervals.
DISCUSSION
MCED model is expected to solve the challenge of “Universal Cancer Screening”
Currently, the published MCED tests are Galleri™ test43, CancerSEEk™ test44, DEEPGEN™ test45, PanSEER test46. cfMeDIP-Seq test47, IvyGene® test48. The most representative of these are CancerSEEk™ test 44,49by Thrive, Inc., developed based on cfDNA and protein-based tumor markers, and Galleri™ test 43 by Grail, Inc., developed based on cfDNA.
It is the emerging MCED test that makes the MCED model a reality. Compared to the SCED model, the MCED model has the following advantages: (1) Having a broader cancer screening spectrum and aggregated prevalence20. (2) Significant improving mental health and decrease subsequent medical costs with reduction in false-positive results20. (3) Having a higher early cancer detection rate50,51. (4) Significantly reduction cancer-specific mortality10,51. (5) Significantly improving the prognosis of cancer patients51 and reducing the cost of cancer treatment 52. (6) More acceptable to the public53.
In fact, the MCED model based on the MCED test may be the only cost-effective screening model for lower-prevalence cancer types9 and is expected to solve the world’s “Universal cancer screening” problem.
The nature of the MCED model
The MCED test treats multiple cancer types as a single disease type, “cancer or malignant tumor”, and converts “multiple screenings for multiple cancers” into “a single screening for multiple cancers”. Compared to the SCED model, which can only screen for a single cancer with conventional imaging (e.g., CT scan of the lungs) or testing products (e.g., blood TPSA), the MCED model can screen for multiple cancers throughout the body with a single MCED test.
All MCED tests screen for cancer via the MCED model. The MCED model is essentially an MCED test that serves as the “first screening”, which is followed by the “final screening”. In short, the MCED test as the “first screening” unifies multiple cancer types into a single disease type of “cancer or malignant tumor”; The MCED test only determines “whether it is cancer”, not “where it is located”. A “negative” result of the MCED test ends the screening, and a “positive” result is followed by “final screening” to determine “where the cancer is located.”
The “first screening” of the MCED model is an MCED test, such as the CancerSEEK™ test, the Galleri™ test, the “YiDiXie™ test”, etc. The “final screening” for the MCED model is a test or group of tests. The “final screening” for the CancerSEEK™ test is PET-CT44. The “Final screening” for Galleri™ test is a self-developed localization system 43, The “final screening” of the “YiDiXie™ test” is a package of routine medical checkups for comprehensive cancer screening (including physical examination, ultrasound, CT, MRI, blood TPSA, etc.).
The rationale behind the development of the two MCED tests
An MCED test is ideal if it has both high sensitivity and high specificity, but sensitivity and specificity of the same test are a contradiction in terms. Therefore, developers often have to balance the pros and cons of prioritizing sensitivity or specificity.
YiDiXie™-HS is optimized for both sensitivity and specificity in the development process. As shown in Table 2, the overall sensitivity of YiDiXie™-HS across cancer types and stages was 90.1% (95% CI: 89.2% - 90.9%; 3971/4405), while the specificity was 89.7% (95% CI: 89.0% - 90.4%; 6002/6689). Thus, YiDiXie™-HS optimally combines sensitivity and specificity.
The development of YiDiXie™-SS, which is an extremely highly sensitive and less specific test, was considered for the following reasons. On the one hand, since a negative result of MCED test will end the screening, false-negative results will lead to missed screening of cancer cases, which are very likely to develop into advanced cancers. Therefore, the sensitivity of the MCED test should be as high as possible to avoid missing cancer patients.
On the other hand, a positive result from the MCED test will lead to “final screening” instead of expensive examinations, invasive procedures, puncture or surgical biopsies, or even incorrect surgical treatments. Therefore, a false-positive result of MCED test does not have the “bad” consequences of over-diagnosis, over-treatment, invasive examination, etc., but rather the only consequence is that the (affordable and non-invasive) “final Screening” is done for nothing. Therefore, the sensitivity of a MCED test is much more important than the specificity.
Therefore, YiDiXie™-SS was developed, which is extremely highly sensitive but less specific. YiDiXie™-SS dramatically increases the number of miRNA markers to achieve extremely high sensitivity to all cancer types. As shown in Table 4, the overall sensitivity of YiDiXie™-SS for different cancer types and stages was 99.1% (95% CI: 98.8% - 99.3%; 4365/4405); the specificity was 65.2% (95% CI: 64.0% - 66.3%; 4358/6689). 3895/6005). YiDiXie™-SS well fulfills the development intent.
YiDiXie™-SS test can replace existing cancer screening tests
Since patients with early-stage cancers missed during cancer screening are very likely to develop advanced cancers, the only alternative to existing cancer screening tests is the MCED test, which is highly sensitive to all clinical stages of all cancer types, including early-stage cancers.
YiDiXie™-SS had an overall sensitivity of 99.1% (95% CI: 98.8% - 99.3%; 4365/4405) for the malignant tumor group (Table 4), with high sensitivity for all clinical stages: stage I, 98.6% (98.0% - 99.1%); stage II, 99.5% (98.9% - 99.8%); stage III, 99.5% (98.6% - 99.8%); stage IV, 99.8% (98.9% - 99.8%) (Table 5); while the total sensitivity of YiDiXie™-HS test for the malignant tumor group was 90.1% (95% CI: 89.2% - 90.9%; 3971/4405) (Table 2), and the sensitivity was high for all clinical stages: stage I, 85.6% (83.9% - 87.1%); stage II, 91.4% (89.6% - 93.0%); stage III, 93.9% (92.0% - 95.4%); and stage IV, 98.4% (96.9% - 99.2%) (Table 3).
Consequently, YiDiXie™-SS can replace existing cancer screening tests, while YiDiXie™-HS is more suitable as a powerful supplement to existing cancer screening tests.
YiDiXie™-SS is expected to solve the world problem of “Universal cancer screening”
Firstly, YiDiXie™-SS can realize the early detection for all cancer types and all clinical stages. The malignant tumor group includes all malignant tumor types (including all solid and hematologic malignant tumors) covered in the “China cancer registry annual report” by the National Cancer Center of China. The total sensitivity of YiDiXie™-SS for the malignant tumor group was 99.1% (95% CI: 98.8% - 99.3%; 4365/4405) (Table 4), and the sensitivity was very high for each clinical stage: stage I, 98.6% (98.0% - 99.1%); stage II, 99.5% (98.9% - 99.8%); stage III, 99.5% (98.6% - 99.8%); stage IV, 99.8% (98.9% - 100.0%) (Table 5). Hence, YiDiXie™-SS can realize the early collection by medical staff. Therefore, the “YiDiXie™ test” allows for cancer screening without having to leave one’s home.
Finally, YiDiXie™-SS has a nearly unlimited detection for all types of cancer and all clinical stages.
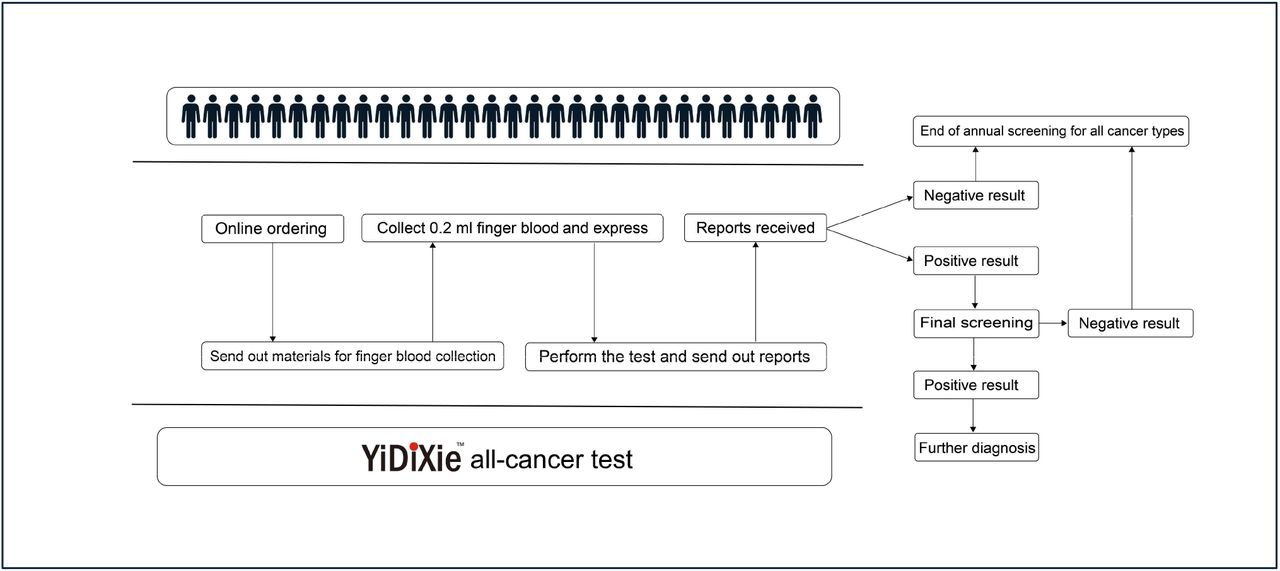
Secondly, the “YiDiXie™ test” requires only a tiny amount of blood, allowing for cancer screening without having to leave one’s home. Only 20 microliters of serum is required to complete a “YiDiXie™ test”, which is equivalent to the volume of 1 drop of whole blood (1 drop of whole blood is about 50 microliters, which produces 20-25 microliters of serum). Considering the pre-test sample quality assessment and 2-3 repetitions of the test, 0.2 ml of whole blood is sufficient to complete the “YiDiXie™ test”. A normal subject can collect 0.2 ml of finger blood at home using a finger blood collection needle without venous blood cancer screening capacity, allowing for “Universal cancer screening” once a year. The traditional SCED model, whose screening capacity is directly dependent on the number of doctors and equipment, makes it almost impossible to realize “Universal cancer screening” once a year for most cancer types. Figure 6 shows the basic flowchart of the “YiDiXie™ test”, which shows that the “YiDiXie™ test” does not require not only doctors and medical equipment, but also medical personnel to collect blood. The patient only needs to place an order online, collect 0.2 ml of finger blood at home, and express it to the laboratory to complete the “YiDiXie™ test”. Thus, YiDiXie™-SS enables “Universal cancer screening” once a year.

Basic flowchart of the “YiDiXie™ test”.
Limitations of the study
First of all, The normal control group were the medical examiners who underwent health checkups. The normal control group subjects were not followed up for more than 1 year, so there must be some malignant tumors hidden among them. As a result, the false-positive rate was higher than the actual situation, resulting in a certain bias.
Second, this study was a case-control study, not a cross-sectional study of the normal population. Therefore, this study cannot demonstrate the positive and negative predictive values of the “YiDiXie™ test” in screening for all malignant tumor types in normal populations.
Final, this study was a single-center, observational study, which could be subject to some bias. In future, multi-center, randomized controlled trials are needed to further evaluate the performance of the “YiDiXie™ test” in screening for all malignant tumor types in normal populations.
CONCLUSION
YiDiXie™-HS has a high sensitivity in all clinical stages of all cancer types and can be a powerful complement to existing cancer screening tests. YiDiXie™-SS has an extremely high sensitivity in all clinical stages of all cancer types and is expected to solve the world problem of “Universal cancer screening”.
Data Availability
All data produced in the present study are contained in the manuscript.
FUNDING
This study was supported by Shenzhen High-level Hospital Construction Fund, Clinical Research Project of Peking University Shenzhen Hospital (LCYJ2020002, LCYJ2020015, LCYJ2020020, LCYJ2017001).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}