
Abstract
Background and Hypothesis Studies on schizophrenia feature diffusion magnetic resonance imaging (dMRI) to investigate white matter (WM) anomalies. The heterogeneity in the possible interpretations of these metrics highlights the importance of increasing their specificity. Here, we characterize WM pathology in early psychosis (EP) and schizophrenia (SZ) with increased specificity using advanced dMRI metrics: Diffusion Kurtosis Imaging and White Matter Track Integrity – Watson (WMTI-W) biophysical model. This enables us to better characterize WM abnormalities and relate them to the patient’s symptomatology.
Study Design dMRI-derived microstructure features were extracted from all of WM and from individual tracts in 275 individuals. 93 patients with EP and 47 with SZ were compared respectively to 135 age-range matched healthy controls (HC). The relationships between the dMRI metrics in WM and various clinical scales were investigated in each patient group.
Study Results WM diffusivities were higher, while kurtosis was lower in EP and SZ vs HC. Differences were more pronounced in EP than SZ. WMTI-W model parameters suggest alterations to the extra-axonal compartment in EP and SZ, consistent with abnormal myelin integrity and WM deterioration. Patient groups showed clustered but non-significant correlations between dMRI metrics and psychotic symptoms. Depressive dimensions were significantly associated with decreased diffusivities in WM, while manic scales correlated with increased diffusivities and reduced kurtosis.
Conclusions dMRI patterns in EP and SZ highly suggest WM deterioration in comparison to HC. DMRI changes better align with affective dimensions, while the relationship with psychotic symptoms may be confounded by competing pathological effects on the microstructure and disease heterogeneity.
Introduction
Positive and negative symptoms are the core characteristics for the diagnosis of schizophrenia (SZ) and other psychotic disorders. The former include delusions and hallucinations, and the latter encompass diminished emotional expression and avolition1,2. Nonetheless, an overlap between the clinical phenotypes of psychosis and mood disorders exists3, leading to a subset of psychosis patients to suffer from mood disorder symptoms and vice versa. Many clinical studies used diffusion magnetic resonance imaging (dMRI) and reported pathological white matter (WM) as a common feature of the disturbances of the psychosis spectrum4–11. The great majority of these studies focus on Diffusion Tensor Imaging (DTI) and its scalar metrics: the most frequently reported and accepted dMRI patterns are reduced fractional anisotropy (FA) and increased mean diffusivity (MD) in patients with chronic SZ4,6,7,10,12,13 and early psychosis4,6–8,14–18 (EP), often reported widespread but with limited spatial consistency4,5,10,19. Such heterogeneity may arise not only from the patients themselves19 but also from different pathological processes affecting the WM, with tracts showing non-degenerating early maturational shifts, or displaying accelerated aging5. Postmortem studies further substantiate the WM involvement found in first episode patients20 and in SZ, reporting myelinated fiber pathology together with dystrophic oligodendroglia21–24 and microglia25.
Several relationships between psychopathological scores and dMRI measures have also been reported but remain unclear. Positive associations have been found between FA and positive symptoms14,26,27, while FA and MD were inversely related to negative symptoms severity7,26. In contrast, other studies reported positive correlation between FA and negative symptoms in the corpus callosum28 as well as anti-correlation between positive symptom and FA in the forceps minor29. Finally, one meta-analysis reported no significant association between symptoms and dMRI metrics10.
Changes in FA and MD can be the consequence of several possible pathological mechanisms like edema30, demyelination31,32, axonal loss or their combination33–35. The heterogeneity in the possible interpretations highlights the importance of increasing the specificity of available in vivo dMRI-derived microstructure metrics by studying the radial and axial diffusivity estimates of DTI, which are rarely reported4,5,9,15,27,36, and estimate Diffusion Kurtosis Imaging37,38 (DKI), an extension of DTI. DKI provides complementary information about tissue heterogeneity at the mesoscale level by quantifying non-Gaussian diffusion arising from heterogeneous diffusion sub-domains within the voxel. DKI has been able to detect widespread WM abnormality39 in regions with complex fiber arrangement40, and subtle abnormalities in subjects at high risk for psychosis41. Nevertheless, DTI and DKI metrics are only sensitive to features of the tissue microstructure. To gain specificity, WM biophysical models of diffusion can be used42. Examples of biophysical model applications to EP and SZ are free-water imaging43 (FWI) and Neurite Orientation Dispersion and Density Imaging44 (NODDI). Most FWI studies reported a global increase in free-water (FW) in SZ45 and across lifespan46 (15–58 years). NODDI detected decreased neurite density (ND) and increased orientation dispersion index (ODI) in first episode47,48 and in patients with SZ49. However, both models showed limitations in terms of ad hoc simplifying assumptions and fit constraints, strongly limiting the interpretability of the microstructure parameters estimated from the data42,50.
In this work we use a more comprehensive biophysical model: White Matter Track Integrity-Watson51–53 (WMTI-W, Fig. 1). WMTI-W features two non-exchanging compartments allowing the estimation of intra- and extra-axonal specific diffusivities that are excellent proxies for intra-axonal injury, inflammation and abnormal myelin integrity respectively34,42,52. WMTI and WMTI-W have been recently used to characterize WM pathology in a variety of patient populations54,55 and animal models of disease31,32, ranging from Alzheimer’s disease56–58 to traumatic brain injury59, but never in schizophrenia. By employing a more comprehensive microstructure model in an exploratory fashion, we aim to characterize for the first time WM pathology in EP and SZ with increased specificity and thus relate it better to the observed symptomatology of our cohort. We hypothesize that this method will overcome the multiple inconsistencies previously found in SZ and in the relation between dMRI metrics and symptom domains.

Schematics of White Matter Track integrity-Watson (WMTI-W) biophysical model. WMTI-W mimics the white matter environment by modelling axons as a collection of sticks. It estimates per voxel: the axonal water fraction f, the intra-axonal diffusivity, Da, the extra-axonal parallel and radial diffusivities, De,// and De,⊥, and the axonal orientation alignment, c2. The extra-axonal compartment is modelled by De,// and De,⊥ and describes the external diffusivities with respect to the main orientation of the axonal bundle. The intra-axonal compartment is modelled as a collection of impermeable zero-radius cylinders, mimicking the WM axons fascicles (sticks), and characterized by the remaining metrics. f measures the proportion of water in the voxel accounted for the WM axons. Da represents the diffusivity within the axons. While c2 quantify how aligned are the axons and it is derived from the concentration parameter of the Watson distribution, k. k is converted to c2 to simplify its interpretation, following: c2 ≡ ⟨cos2ψ⟩, with ψ being the angle between axons and the main bundle orientation. c2 varies between ⅓, isotropic, and 1, perfectly parallel axons.
Methods
Participants
The data used for this study was collected from 275 individuals and divided into three groups: 135 healthy controls (HC), 93 EP and 47 SZ (Table 1). EP patients (within 5 years after a first psychotic episode as defined by the Comprehensive Assessment of At-Risk Mental States scale60, CAARMS) or SZ patients with a DSM-IV diagnosis of schizophrenia and schizoaffective disorder were recruited from the Lausanne University Hospital. EP patients with psychosis related to intoxication, organic brain disease, or IQ<70, were excluded, as well as SZ individuals reporting alcoholism, drug abuse, major somatic disease, documented anamnestic or current organic brain damage. Finally, HC were excluded if they, or a first-degree family member, suffered from psychosis or prodromal symptoms, or reported current or past antipsychotic treatment. The HC group was further subdivided into younger (HC-Y, n=130, age=26.8±6.8) and older (HC-O, n=84, age=31.9±8.1) to better match the age ranges of the two clinical groups (EP=24.7±5.5; SZ=38.1±9.4 years). Participants provided written informed consents. The study was conducted in accordance with the Declaration of Helsinki and approved by the local Ethics Committee of the Canton of Vaud (Switzerland) under authorization numbers CER-VD 382/11 and 2018-01731. Within-group individual diagnoses are reported in Supplementary Table S1.
P-values refer to Wilcox’s tests between clinical and healthy control groups. χ2 test is computed for the whole scanner and sex contingency table. HC: healthy controls, Y: young, O: old, EP: early psychosis, SZ: chronic schizophrenic, Delta MRI-Clin. Ass.: difference in months between MRI scan and clinical assessment, SOFAS: Social and Occupational Functioning Assessment Scale, GAF: Global Assessment of Functioning, PANSS: Positive and Negative Syndrome Scale, MADRS: Montgomery-Asberg Depression Rating Scale, YMRS the Young Mania Rating Scale.
MRI acquisition
MRI scanning sessions were performed on two different 3-Tesla systems (Magnetom TrioTim and PRISMA, Siemens Healthineers, Erlangen, Germany), each equipped with a 32-channel head coil. A 1-mm isotropic T1-weighted image was acquired for anatomical reference. Whole-brain diffusion-weighted images (DWI) were acquired using diffusion spectrum imaging (DSI) scheme across 15 b-values, ranging from 0 to 8000 s/mm2, voxel size of 2.2 x 2.2 x 3 mm3. Further information can be found in the acquisition details section of the Supplementary Material.
Image preprocessing
The MPRAGE image was bias field corrected61 and skull-stripped via nonlinear registration to the MNI-152 template62 using Advanced Normalization Tools63 (ANTs). The diffusion preprocessing pipeline included MP-PCA denoising, Gibbs ringing-, EPI-, eddy current and motion corrections, following most recent guidelines64 - see Supplementary Material for preprocessing details.
Microstructure estimation
For DKI and WMTI-W estimation, the diffusion dataset was truncated at b≤2500 s/mm2 (Jensen et al., 2005). DKI was fit voxel-wise in the entire brain65 using Matlab, from which seven parameter maps were derived: four from DTI: radial, mean, axial diffusivity (RD, MD, AD) and fractional anisotropy (FA), and three from DKI: radial, mean, axial kurtosis (RK, MK, AK). Then, WMTI-W model parameters were estimated voxel-wise from the DTI and DKI parameters, using an in-house Python script, yielding other five parameter maps: axonal density f, intra-axonal diffusivity Da, extra-axonal parallel and perpendicular diffusivities De,//, De,⊥ and axon orientation alignment c2 (Fig. 1). The WM characterization thus relied on 12 microstructure metrics.
ROI analysis
Individual FA maps were non-linearly registered to the Johns Hopkins University FA template66 (JHU) using ANTs, and the WM region-of-interest (ROI) labels from the template were then mapped back to individual space using the resulting spatial transformations. The mean value of each microstructure metric was computed inside each ROI and their ensemble (whole JHU-defined WM, from here on referred to as core of the WM).
Psychiatric scales
Level of functioning was assessed with the Global Assessment of Functioning67 scale (GAF). Symptom levels were measured with the Positive and Negative Syndrome Scale68 (PANSS), the Montgomery-Asberg Depression Rating Scale69 (MADRS) and the Young Mania Rating Scale70 (YMRS). For the PANSS, items were categorized using the Wallwork/Fortgang five-factor model71 (WW) which comprises five dimensions: positive (pos.), negative (neg.), disorganized (dis.), depressive (depr.) and excited dimension (exc.). PANSS data was not available for 5 EP and 1 SZ subjects, MADRS and YMRS were not assessed in 6 EP and 16 SZ subjects.
Statistical analysis
Before any statistical analysis, all the microstructure parameter estimates in the WM core and individual JHU ROIs were harmonized for scanner type via ComBat harmonization72 that has proven efficient at correcting scanner effects in the same cohort73. Distributions for each metric, ROI and group were tested for normality using the Shapiro–Wilk test74 and for homogeneity of variance using the Levene’s Test75. The statistical test used for group comparisons was chosen based on distribution characteristics, resulting in dMRI metrics for the WM core being tested via non-parametric Wilcoxon signed-rank76 test, suitable for non-normal but homogeneous variance distributions. At the ROI level, dMRI metrics between groups were compared using the non-parametric Brunner-Munzel77,78 test, suitable for distributions with unequal variances. In all comparisons, the estimates were controlled for sex and quadratic5 age, and p-values were false discovery rate (FDR) corrected. The model selection procedure for age correction is reported in the age correction section of the supplementary material and plot in Supplementary Figure S1. The dice coefficient was used to quantify the similarity in ROI alterations across the brain, indicating the proportion (between 0 and 1) of significant alterations that EP and SZ groups have in common.
Microstructure metrics in the WM core were correlated to psychiatric scales. The correlation matrices for EP and SZ were analyzed via hierarchical clustering (distance: euclidean; clustering method: complete linkage; dist, hclust functions in R79) and p-values were FDR-corrected. Finally, the individual correlations that remained significant were further investigated via robust regression (robustbase80,81), to ensure robustness to outliers, and a second correlation analysis was performed to determine which JHU ROIs contributed the most to the significant association in the whole WM core.
Results
Cohort demographics
The cohort demographics are displayed in Table 1. Significant differences were found in age between groups (p<.0001), leading to the inclusion of age as a covariate. Significant differences between EP and SZ were found in the illness duration (p<.0001) but not in the age at onset or CPZ-equivalent dose.
Diffusion kurtosis and microstructure imaging estimates
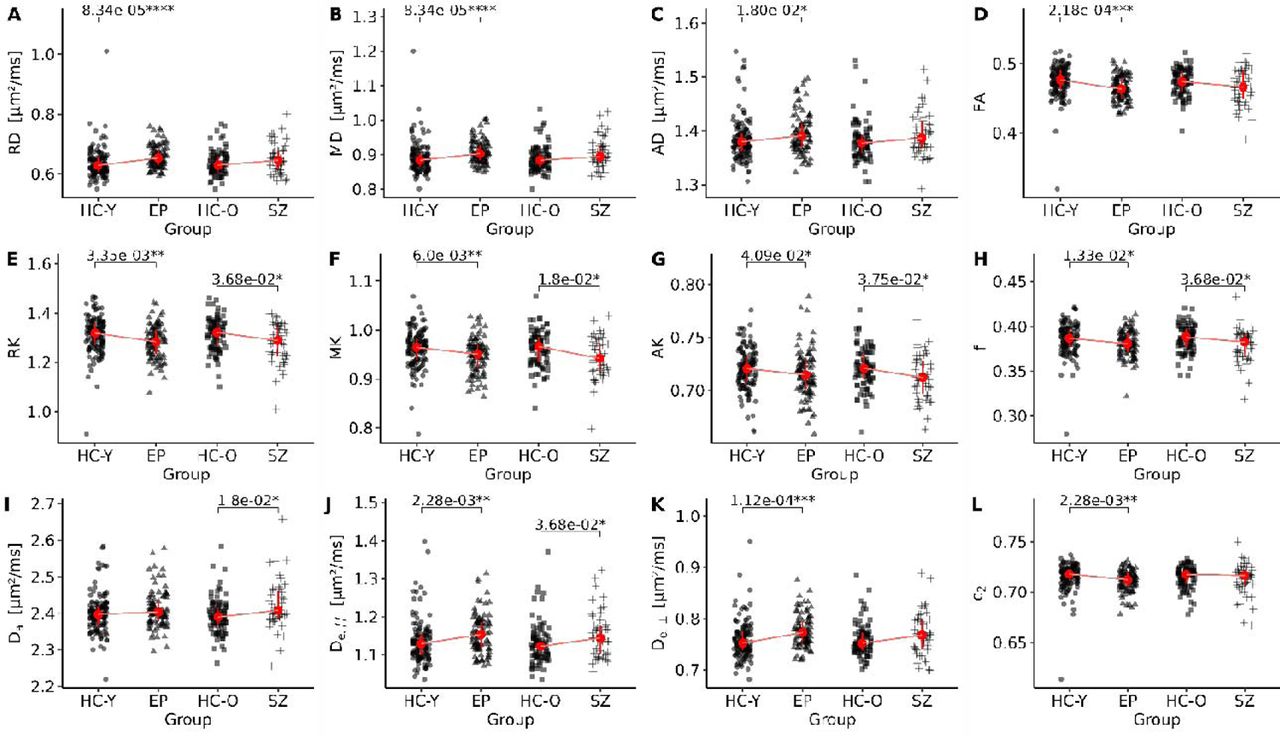
The estimated study templates for DTI, DKI and WMTI-W metrics are plotted in Fig. S2. The harmonized mean estimates of the WM core are reported for the four distinct groups in Table S2. In the WM core, several group differences were found (Fig. 2). Compared to HC-Y, EP showed significantly higher DTI diffusivities and lower FA (Fig. 2A to D; RD, MD: p<.0001, FA: p=.00021, AD: p=.018), as well as lower kurtosis (Fig. 2E, F, G; RK: p=.0035, MK: p=.0060; AK: p=.041). Axonal water fraction, f, and alignment, c2, in EP were also significantly lower than in HC-Y (Fig. 2H, L; f: p=.013 c2: p=.0022), while extra-axonal diffusivities, De,// and De,⊥, were higher (Fig. 2J, K; De,//: p=.0022, De,⊥: p=.00011). No significant differences were found between EP and HC-Y in terms of intra-axonal diffusivity Da (Fig. 2I). Differences between SZ and HC-O were more limited, with no differences at the level of DTI metrics. Kurtosis, however, was also lower in SZ (Fig. 2E, F, G; RK: p=.036, MK: p=.018, AK: p=.037). The WMTI-W metrics showing significant differences were reduced f (Fig. 2H; p=.036), increased Da (Fig. 3I; p=.018) and De,// (Fig. 2J, p=.036). Numeric p-values, effect sizes, and confidence intervals can be found in Table S3. We found no significant differences between EP and SZ (see Table S4).

Strip plot of the group comparisons. Each clinical group is compared to its respective HC group. EP: early psychosis, SZ: chronic schizophrenic, HC-Y/O: healthy controls young/old. *:p≤5e-2, **:p≤1e-2, ***:p≤1e-3, ****:p≤1e-4.

Heatmap of the ROI group comparison. Group comparisons (y-axis right) heatmap of the Brunner-Munzel test significance levels for each dMRI metric (y-axis left) and each region of interest (x-axis). Red: clinical group has higher value than the HC, Blue indicates the opposites. The darker the color, the lower is the p-value; ns: p≤1, *:p≤5e-2, **:p≤1e-2, ***:p≤1e-3, ****:p≤1e-4. Abbreviations: EP: early psychosis; HC-Y/O: younger/older healthy control; SZ: chronic schizophrenia; L: left; R: right; MIDCP: Middle cerebellar peduncle; PCT: Pontine crossing tract (a part of MC; GCC: Genu of corpus callosum; BCC: Body of corpus callosum; SCC: Splenium of corpus callosum; FX: Fornix (column and body of fornix; CST: Corticospinal tract; ML: Medial lemniscus; ICP: Inferior cerebellar peduncle; SCP: Superior cerebellar peduncle; CP: Cerebral peduncle; ALIC: Anterior limb of internal capsule; PLIC: Posterior limb of internal capsule; RPIC: Retrolenticular part of internal capsule; ACR: Anterior corona radiata; SCR: Superior corona radiata; PCR: Posterior corona radiata; PTR: Posterior thalamic radiation (include optic radiation); SAGSTR: Sagittal stratum; EC: External capsule; CING/CG: Cingulum (cingulate gyrus); CING/HIP: Cingulum (hippocampus); FX/STRIA: Fornix (cres) / Stria terminalis; SLF: Superior longitudinal fasciculus; SFOF: Superior fronto-occipital fasciculus; IFOF: Inferior fronto-occipital fasciculus; UF: Uncinate fasciculus; TPTM: Tapetum.
Group comparison of the JHU ROIs revealed distinct patterns in the dMRI metrics tendencies, highlighting ROI specific alterations in both EP and SZ (Fig. 3). Most affected bundles included the corpus callosum (CC), fornix (FX), corona radiata (CR), posterior thalamic radiation (PTR), sagittal stratum (SAGSTR), cingulum (CING/CG) and superior longitudinal fasciculus (SLF).
Common features were higher DTI diffusivities in both EP and SZ with respect to their HC groups, with the EP group having the most distinct and widespread increase across the WM. We quantified the percentages of WM ROIs with higher RD, MD, and AD, respectively: 56, 54, 18% in EP and 12, 16, 8% in SZ (Fig. 3, both DTI sections, in red). These differences were generally paired to lower FA of the same ROI in EP, but not as consistently in SZ (34 vs 4%; Fig. 3, both blocks, FA in DTI sections).
Kurtosis metrics were lower in both patient groups (Fig. 3, both DKI sections, in blue). In EP, the significantly lower DKI metrics were matched to the changes in DTI metrics except for the bilateral cerebellar peduncle (CP) and CING (hippocampal section acc. JHU) areas. Decreased kurtosis was significant for RK, MK and AK in 24%, 34% and 20% of ROIs, respectively (Fig. 3, upper-block, DKI section, in blue). In SZ patients, this trend was notably less consistent (RK: 20%, MK: 24%, AK: 12% of ROIs; Fig. 3, bottom-block, DKI section, in blue), with some ROIs showing alterations detected by DKI and not DTI, such as the bilateral SAGSTR, the left anterior limb of internal capsule (ALIC) and FX and vice versa, e.g. in CING and right anterior corona radiata (ACR). WMTI-W metrics display the same trends as for the whole WM analysis, with f lower in several locations of the WM in SZ and especially EP (10% vs 18% of ROIs, Fig. 3, WMTI sections, in blue), and higher extra-axonal diffusivities. In EP, De,// and De,⊥were significantly altered in 24 and 20% of the ROIs respectively. In the SZ group, De,// and De,⊥ showed fewer number of significant alterations, 16% and 6%. Notably, Da alterations were uncommon in both groups and not spatially consistent. Finally, sparse c2 alterations were found in EP (6% of ROIs) but none in SZ (Fig. 3, both blocks, WMTI section, in red). Overall, the Dice coefficient between EP and SZ differences to their respective HC (heatmaps) was 0.36, measuring the agreement across altered ROIs. For additional details about FDR p-values, effect size and confidence intervals see Table S5 and Table S6.
Association between microstructure estimates and psychopathological symptom domains
Differences in psychiatric scales between EP and SZ can be found in Table 1. We correlated psychiatric scores to microstructure metrics in the whole WM core because dMRI metrics showed consistent changes across JHU ROIs and this approach limited the number of statistical tests.
Overall, correlations between psychiatric scales and dMRI metrics in WM were stronger in SZ than EP (Fig. 4A vs B). In both groups, hierarchical clustering identified three macro clusters in dMRI metrics (Fig. 4A, B top dendrograms and vertical columns): i) diffusivities (RD, MD, AD, De,//, De,⊥, Da), ii) variance within voxels informing about the tissue complexity (RK, AK, MK, f), and iii) axonal bundle anisotropy (FA, c2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hierarchical clustering of the correlation matrices between white matter microstructure estimates and psychopathological symptoms domains. The plot is divided into EP (A, left) and SZ (B, right) groups. Colors mark the Pearson correlation coefficient value (intensity) and positive (red) or negative (blue) direction of the association. The smaller cluster subdivisions indicate clusters of interests. Asterisks indicate those correlations whose FDR-corrected p-value is significant (FDR<.05). GAF: Global Assessment of Functioning scale; MADRS: Montgomery-Asberg Depression Rating Scale; YNRS: Young Mania Rating Scale; WW: Wallwork five-factor model for the Positive and Negative Syndrome Scale; pos.: positive; neg.: negative (neg.), dis.: disorganized; depr.: depressive; exc.: excited/manic dimension.
The clustering of psychiatric dimensions revealed patterns of correlation between dMRI metrics and psychiatric scales within the clinical groups, particularly in SZ. In EP, psychiatric dimensions were classified into three clusters (Fig. 4A, Dimensions, left dendrogram). The first cluster, which included GAF, WW neg. and WW dis., showed weak pattern of correlations with dMRI metrics. The second cluster, which included WW pos. and YMRS, (Fig. 4A), showed a selective positive association with the WM complexity metrics and weak negative correlations with the tissue diffusivities. The third cluster, which grouped affective symptoms (WW exc., WW depr. and MADRS) was characterized by negative associations with the tissue diffusivities and positive with complexity metrics (Fig. 4A). However, only the correlations of lower MD and RD with higher WW depr. score, were significant after FDR correction.
In SZ, the clustering of the symptom dimensions differed from that of EP (Fig. 4B). A first cluster was found for manic behaviors, where YMRS and WW exc. scores correlated with increased dispersion (lower FA, c2), increased diffusivities, and decreased complexity metrics (Fig. 4B, first cluster), opposite of EP trends for the same dimensions. YMRS correlations to FA, c2, MD, RD, and De,⊥ remained significant after FDR correction. A second cluster comprising WW neg., pos., and dis. was characterized by negative associations with anisotropy metrics (FA, c2), and positive associations with complexity metrics. In this cluster, WW dis. showed stronger association to kurtosis, f and c2 than WW neg and pos. Finally, the third cluster which included depressive symptoms (WW depr. and MADRS) and GAF, primarily shared a consistent negative correlation with complexity metrics (Fig. 4B). Notably, the axonal anisotropy metrics, FA and c2, were the measures that showed the most consistent correlations among the symptom dimensions in SZ.
To further analyze the correlations between dMRI metrics and psychiatric scales, we plotted those correlations that survived multiple comparison correction (identified by an asterisk in Fig. 4A, B). Robust regression analysis yielded correlation coefficients of r=-.26 (p=.015) and r=-.24 (p=.037), between the WW depressed factor and AD and MD, respectively, in EP (Fig. S3A, B). The ROI-wise correlation analysis revealed that the body of the corpus callosum (BCC), right superior CP, superior CR, and right cingulum (CING) were the ROIs mostly driving these significant associations (Fig. S6A).
In SZ, YMRS total (Fig. 4B) score was the dimension which significantly correlated with the highest number of dMRI metrics. These metrics were MD (r=.47, p=.0012; Fig. S5A), RD (r=.55, p=.0015; Fig. S5B), De,⊥, (r=.60, p=.0059; Fig. S5D), FA (r=-.60, p=.0024; Fig. S5C) and the axonal orientation alignment c2 (r=-.66, p=.017; Fig. S5E). However, we could not find a subgroup or specific YMRS items that could unambiguously explain these findings and, overall, SZ patients in our cohort did not score beyond the YMRS remission threshold (YMRS total score ≤12). To try to further understand our findings, we tested the individual items defining the WW exc. (PANSS P4-excitement, P7-hostility, G8-uncooperativeness and G14-impulse control71), which was clustered with the YMRS scale. We found that only the P4-excitement item significantly correlated (after FDR correction) to RD (r=.41, p=.012), MD (r=.38, p=.020), FA (r=-.40, p=.013) and De,⊥ (r=.40,p=.012. The ROI-wise correlation analysis revealed widespread associations of the YMRS scores across the WM (Fig. S6B), including CC, sections of the bilateral CP, bilateral ALIC, the entirety of the CR, PTR, SAGSTR, left EC, fornix/stria (FX/STRIA), superior and inferior fronto-occipital fasciculus (SFOF, IFOF) and uncinate fasciculus (UF). Finally, the significant negative association between the WW disorganized factor and c2 in SZ (r=-.56, p=.023) is plotted in Fig. S4. In a similar fashion to the YMRS, the JHU ROI c2 associations with the WW dis. factor were numerous, affecting bilaterally the CP, the ACR and the EC (Fig. S6B).
Discussion
With the present analysis we employed more advanced diffusion metrics than DTI, namely DKI and a comprehensive microstructure model, WMTI-W, both aimed at characterizing the WM pathology with increased sensitivity and specificity in our early psychosis and schizophrenia cohorts.
Our findings reveal that WM alterations as assessed using dMRI microstructure metrics are already present and widespread in the EP stage and differences in microstructure are less pronounced between chronic SZ and HC-O when accounting for age. Furthermore, most EP and SZ WM differences to HC concern the radial direction of diffusion, i.e., perpendicularly to the bundle main axis. Thus, RD and MD were the most affected, while AD differences were less significant. Our study confirms previous DTI5,15,16,82, dMRI microstructure73,83 and post-mortem cytoarchitectural20 alterations found already at the EP stage, and the widespread reduced FA and increased MD4–8,12,14–16,18,48, RD and AD8,13,84,85 in areas commonly reported in EP and chronic SZ.
In addition, WM kurtosis was lower for both patient groups, but also more pronounced in EP, and more particularly in the radial direction (RK: 24% vs 20%, AK: 20% vs 12% of ROIs), representing a decrease in tissue complexity and heterogeneity34,37,38,86. Remarkably, in SZ vs HC-O, DKI was able to identify differences in WM ROIs (SAGSTR, left ALIC and FX) that were not evident in DTI. In a review from Pasternak et al.87, all studies but one also reported reduced MK, with one study also reporting lower RK and AK in SZ patients40.
Our ROI-specific differences in dMRI metrics between patients and controls were consistent with literature, as previous studies also reported alterations in CING5, FX88,89, CR90–92, PTR92,93 and SAGSTR93 in EP, that remained present in SZ patients. CC and SLF5,7 are considered to have a declining trajectory with aging in SZ5,7 (either FA decrease or MD increase when compared to HC), but our results confirm only the SLF trajectory (increased MD, decreased FA in EP and decreased kurtosis in SZ), while the CC was not altered as much in SZ as in EP5,88–93.
For the first time, we used WMTI-W, a comprehensive biophysical model of WM, to tease apart possible pathological contributions to the reported WM differences. In EP, WMTI-W helps attribute the observed alterations to the extra-axonal compartment, due to the significant increase in De,// and De,⊥, but not Da. The lower axonal water fraction f and orientation coherence c2 are further consistent with pathological features such as reduced myelination and axonal density. The former have indeed been shown to induce an increase in De,⊥ and decrease in f (e.g. in mouse model of cuprizone demyelination31,32) while the increase in De,// can be a consequence of overall reduced cellular density and thereby hindrance in the extra-axonal space. The SZ group was overall characterized by higher De,// and lower f, also pointing to less densely packed extra-cellular space. The WM core analysis suggested also higher intra-axonal diffusivity Da in this group, but only two specific ROIs sustained this trend (CING and CC). Previous works using NODDI44, a comparable but more constrained biophysical model, also reported reduced neurite density (ND, comparable to f) in several ROIs and increased orientation dispersion index (ODI, corresponding to lower c2) in both first episode and chronic patients83. These patterns of preferentially altered extra-axonal environment are also consistent with reports of global increase in “free water” using the FWI technique in SZ cohorts45, although FWI conflates potential pathological mechanisms by defining a tissue compartment (intra- and extra-axonal) vs a free water (cerebral spinal fluid) one.
Pathological WM changes identified using WMTI-W are further supported by neuroimaging findings beyond dMRI, such as a 14% reduction in WM volume94, and ultrastructural post-mortem studies reporting myelinated WM fiber pathology, mainly consequence of the decompacting and splitting of the myelin sheath, but also the inclusions of vacuoles in between myelin layers, small-axons atrophy, and the presence of swollen or dystrophic oligodendroglia22–24 and microglia25. In parallel to these morphological changes, a 27-28% reduction in oligodendrocyte densities were reported in cortical layer III and subcortical areas21 of SZ brains. Despite these histological analyses focused on the frontal brain regions21–23,25 and on older patients and the postmortem nature of the examination, the pathological WM changes they report agree with changes evidenced by the whole-brain dMRI analysis and by the WMTI-W model microstructure parameters in the present study. Going forward, dMRI combined with careful biophysical modeling could continue to provide crucial information about cellular-level brain changes in EP and SZ in vivo and longitudinally.
The clustering of behavioral scales in the regression analysis with dMRI metrics revealed that most correlations between WM microstructure and symptomatology were weak and non-significant. Second, the affective dimensions correlated better with changes in WM microstructure, and these associations were more significant in the SZ cohort. Third, a set of within-group associations were in contrast with the microstructure group comparisons to age range-matched HC. Namely, opposite to the higher diffusivities, reduced kurtosis and reduced f found between SZ and HC, the cluster containing WW neg.-pos.-dis. showed a positive score association with complexity metrics (kurtosis, f) in SZ. A similar associative pattern was found in EP for the WW pos.-YMRS and WW depr.-exc.-MADRS clusters, that showed respectively a positive score association with complexity metrics (kurtosis, f), and a negative score association with diffusivities. Thus, worse symptoms on some of these scales within a given patient group were mirrored by WM changes opposite of those found from the comparison to HC. This scenario could be caused by either the patient heterogeneity, especially in the EP group, or competing pathological mechanisms of deterioration5-abnormal myelination31 vs neuroinflammation34 that have opposite effects on dMRI metrics and, when combined, result in a more challenging interpretation. Indeed, neuroinflammation has the effect of reducing diffusivities and increasing kurtosis due to higher cellular crowding associated with microgliosis and astrocytosis31,32,34,35. In support of this mechanism, proinflammatory cytokines have been reported to be elevated in EP95 and SZ96, and related to negative symptoms in EP95.
However, when examining closely the correlation of stronger depressive symptoms to lower MD and AD in EP, patients with low scores on these scales displayed elevated diffusivities compared to the HC-Y mean, consistent with EP to HC-Y group differences, while patients with high depressive scores displayed similar WM diffusivities to HC-Y. These results are consistent with reports that higher depressive dimensional scores were sometimes associated to fewer hospitalizations and fewer relapses at 3 and 5 years97, indicating better outcome for these patients, although poorer prognosis was also often reported98. Furthermore, the ROIs driving this correlation (CC, CR, CING) are often highlighted in WM DTI studies of depression99.
In SZ, a worse WW dis. score was found associated to worse fiber coherence, consistent with the group comparison results. Furthermore, lower score patients displayed c2 values like those of HC-O, which diverged as the score increased. In the literature about SZ, disorganized symptoms have been related to decreased FA in the ACR91 and cingulum100 (similar to our findings), increased MD of the longitudinal fasciculus7 and worse cognitive impairment101.
Finally, when considering excitement and manic behavior, worse scores within the SZ group correlated with the signature of deteriorated WM, i.e., increased diffusivities, reduced kurtosis and were thus consistent with the SZ to HC-O group differences. The YMRS total score was found to be significantly associated with higher diffusivities and lower anisotropy, but also decreased complexity metrics, attributed to higher excitement symptoms, and diverging from HC-O as the score worsened. In the literature, findings have reported that the worsening of the disease was associated with impulsivity, aggression22,102,103 and, in EP, higher excitement scores led to poorer prognosis97. Among the many ROIs contributing to these results, the most consistent were localized in the frontal regions (GCC, ALIC, ACR, UF), possibly related to the reported abnormal frontal activity associated with excitement symptoms in patients with SZ104.
The first limitation of the present study is the heterogeneity of the patient cohorts, which may explain the weak relationships between the symptomatology and WM integrity. Thus, the generalizability of our conclusions needs to be confirmed in other cohorts. Furthermore, as symptoms are transitory in nature, the patient’s symptomatic state at the time of the MRI scan or evaluation may differ from the state that led to the assigned clinical score. This mismatch highlights the challenges of relating brain pathology characterized non-invasively using dMRI to symptomatology and the necessity to embrace different approaches to face such heterogeneity.
In conclusion, with this work we demonstrated that WM alterations, already present at the early psychosis stages, manifest preferentially perpendicularly to the axons as major extra-cellular increase in diffusivities, reduced restricted water, decreased intra-cellular water fraction, and loss of fiber alignment. With time, these changes become less dramatic in chronic SZ as compared to age-matched controls. Finally, the current study is one of the few that reports relationships between symptoms and advanced dMRI brain WM microstructure. At the SZ stage, WM deterioration is linked to stronger excitement and manic scores.
Data Availability
Data is not available for public use.
Acknowledgments
This work was supported by the Swiss National Science Foundation (PCEFP2_194260, to I.J.), the National Center of Competence in Research (NCCR) “SYNAPSY - The Synaptic Bases of Mental Diseases” from the Swiss National Science Foundation (n° 51NF40 – 185897 to KQD & PC) and the Foundation Alamaya. Dr Alameda is supported by Carigest fellowship and by Frutiger Adrian et Simone fellowship. Dr Dwir is supported by Frutiger Adrian et Simone fellowship. The authors have nothing to disclose and there are no conflicts of interest.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵



