
Abstract
The general public are advised to have regular routine eye examinations to check their vision and ocular health; however current UK guidance on how often to have eye examinations is not evidence-based and was issued in 2002.This Rapid Review aims to provide an evidence base that stakeholders can use to form updated guidance for Wales by asking the question ‘What are the prognostic factors for a change in ocular status in the general population attending routine eye examinations?’
The review included evidence available from January 2009 up until August 2023. Evidence was included from 2011 up until 2023. 19 studies were included: two systematic reviews; nine prospective cohort studies; three retrospective cohort studies; two longitudinal studies; two case-control studies; and one cross-sectional study were included.
Research Implications and Evidence Gaps Future research to inform appropriate eye examination intervals should be narrower in focus to ensure as much relevant and useful evidence as possible is gathered. There are large amounts of evidence on prevalence and prognostic factors for prevalent conditions, which did not meet the inclusion criteria of this rapid review which looks at incident or changing conditions.
Policy and Practice Implications Caution should be taken if using this review for decision making on appropriate eye examination intervals due to low certainty and generalisability. This review should be used to identify key prognostic factors and suggesting these for further targeted research and evidence synthesis.
Economic considerations Sight loss costs the UK economy 25 billion pounds per annum, with more than 2 million people in the UK currently living with sight loss. The economic implications of appropriate or inappropriate testing intervals for different causes of vision loss will be different. When captured at a population wide scale, the earlier detection of conditions through examination can result in significant economic savings.
Funding statement The Centre for Health Economics and Medicines Evaluation, the Bangor Institute for Medical and Health Research, and the Swansea Centre for Health Economics were funded for this work by the Health and Care Research Wales Evidence Centre, itself funded by Health and Care Research Wales on behalf of Welsh Government.
EXECUTIVE SUMMARY
What is a Rapid Review?
Our rapid reviews (RR) use a variation of the systematic review approach, abbreviating or omitting some components to generate the evidence to inform stakeholders promptly whilst maintaining attention to bias.
Who is this summary for?
This Rapid Review is intended for use by clinical leaders and decision makers in Wales’ primary eye care services. The evidence in this Review is intended to be used to examine the risk of a person experiencing a change in their ocular health, vision, or systemic health that affects their eyes so that guidance can be produced on how often people should attend for routine eye examinations based on their individual risk factors.
It is also intended to identify gaps in the evidence to determine where further research is required for certain risk factors or patient groups.
Background / Aim of Rapid Review
The general public are advised to have regular routine eye examinations to check their vision and ocular health; however current UK guidance on how often to have eye examinations is not evidence-based and was issued in 2002.
This Rapid Review aims to provide an evidence base that stakeholders can use to form updated guidance for Wales by asking the question “What are the prognostic factors for a change in ocular status in the general population attending routine eye examinations?”
Results
Recency of the evidence base
The review included evidence available from January 2009 up until August 2023. Evidence was included from 2011 up until 2023.
Extent of the evidence base
19 studies were included: two systematic reviews; nine prospective cohort studies; three retrospective cohort studies; two longitudinal studies; two case-control studies; and one cross-sectional study were included.
Key findings and certainty of the evidence
Demographic prognostic factors: age, sex, ethnicity, and household net worth are potential prognostic factors for a change in ocular health or vision.
Ocular prognostic factors: intraocular pressure, family history of glaucoma, visual acuity, visual field mean deviation, spherical equivalent refraction, high myopia, age-related macular degeneration, glaucoma, and cataract are potential prognostic factors for a change in ocular health or vision.
Lifestyle/behaviour prognostic factors: diet, alcohol intake, smoking, time spent outdoors, and time spent reading are potential prognostic factors for a change in ocular health or vision.
Systemic health prognostic factors: hypertension, heart disease, cholesterol, diabetes, peripheral arterial disease, hypercoagulable state, stroke, pregnancy, age at menarche, oral contraceptive use, and atopy are potential prognostic factors for a change in ocular health or vision.
Increasing length of time between eye examinations is a potential prognostic factor for a change in ocular health or vision.
The level of certainty for all prognostic factors is low as there was generally only one study reporting for each individual outcome.
Studies were often performed in specific populations, meaning the results cannot be applied to the general population, particularly due to low study numbers per outcome.
Research Implications and Evidence Gaps
Future research to inform appropriate eye examination intervals should be narrower in focus to ensure as much relevant and useful evidence as possible is gathered. Prognostic factors or specific ocular conditions of interest potentially need to be investigated individually for their effect on a change in ocular status.
There are large amounts of evidence on prevalence and prognostic factors for prevalent conditions, which did not meet the inclusion criteria of this rapid review which looks at incident or changing conditions. Further evidence generation could be conducted in this area.
Very little evidence was identified in a UK setting, more primary evidence generation may be required.
There is a notable lack of evidence in younger adults aged under 40 years.
Policy and Practice Implications
Caution should be taken if using this review for decision making on appropriate eye examination intervals due to low certainty and generalisability.
This review should be used to identify key prognostic factors and suggesting these for further targeted research and evidence synthesis.
Economic considerations
Sight loss costs the UK economy £25 billion per annum, with more than 2 million people in the UK currently living with sight loss.
The economic implications of appropriate or inappropriate testing intervals for different causes of vision loss will be different.
A new case of age-related macular degeneration (AMD) in an adult aged 50 or over, costs the UK economy £73,350 over the person’s lifetime. Lifetime costs to the UK economy for a person diagnosed with glaucoma are approximately £49,800 per person. Reducing the prevalence of these conditions by just 14 or 20 cases respectively could save the UK economy £1 million in lifetime costs.
On economic grounds, early detection of AMD in eye care services and the eye care pathway may be of benefit due to the high level of prevalence and associated long term costs to the NHS as the condition causes irreversible, life limiting damage.
When captured at a population wide scale, the earlier detection of conditions through examination can result in significant economic savings.
Disclaimer: The views expressed in this publication are those of the authors, not necessarily Health and Care Research Wales. The Health and Care Research Wales Evidence Centre and authors of this work declare that they have no conflict of interest.
1. BACKGROUND
1.1 Who is this review for?
This Rapid Review was conducted as part of the Health and Care Research Wales Evidence Centre Work Programme. The original question was suggested by the National Clinical Leads for Wales General Ophthalmic Services and the Optometry and Audiology Policy Branch, Welsh Government. Working with these stakeholders, the question was then amended to the one mentioned above.
This Rapid Review is intended for use by clinical leaders and decision makers in Wales’ primary eye care services. The evidence in this Review is intended to be used to examine the risk of a person experiencing a change in their ocular health, vision, or systemic health that affects their eyes so that guidance can be produced on how often people should attend for routine eye examinations based on their individual risk factors.
It is also intended to identify gaps in the evidence to determine where further research is required for certain risk factors or patient groups.
1.2 Background and purpose of this review
The general public are advised to attend routine eye examinations to regularly check their visual acuity, provide any necessary vision correction, and identify ocular health problems. Current guidance in the UK was issued in 2002 and is based on a consensus decision regarding minimum re-examination intervals, with no evidence base. The currently recommended minimum intervals are:
Under 16 years in the absence of any binocular vision anomaly - 1 year
Under 7 years with binocular vision anomaly or corrected refractive error - 6 months
7 years and over and under 16 with binocular vision anomaly or rapidly progressing myopia - 6 months
16 years and over and under 70 years - 2 years
70 years and over - 1 year
40 years and over with a family history of glaucoma or with ocular hypertension and not in a monitoring scheme - 1 year
Diabetic patients - 1 year
With significant reform of Wales General Ophthalmic Services underway, it is pertinent to review the evidence that is available that may be able to inform recommendations on the frequency of routine eye examinations in Wales.
The evidence identified in this review will be used by stakeholders to help answer questions similar to the below:
What is the risk of an asymptomatic person attending for a routine eye examination having experienced a change in ocular status?
Is there evidence to suggest that this risk may vary between different groups?
Can the evidence regarding this risk be used to inform appropriate time intervals between routine eye examinations?
2. RESULTS
2.1 Overview of the Evidence Base
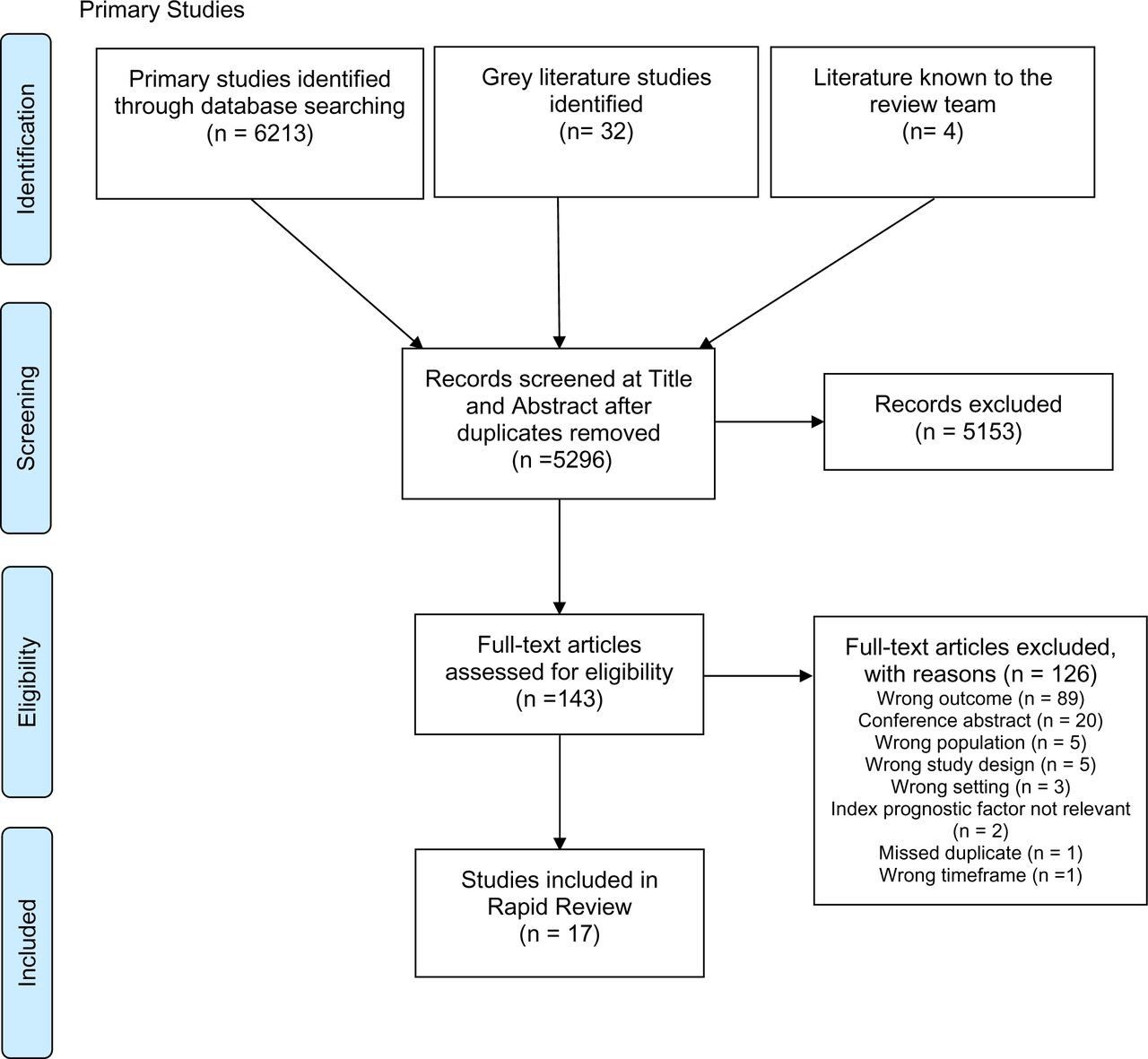
Nineteen studies were identified that met the inclusion criteria of this rapid review. Two systematic reviews and 17 primary studies were included, all of which are observational studies. The study designs varied, with nine prospective cohort studies; three retrospective cohort studies; two longitudinal studies; two case-control studies; and one cross-sectional study included. Sample sizes were also very different across studies, with some having only a few hundred participants whilst others had more than 400,000. Full details of the eligibility criteria are presented in Section 5.1, Table 7. Full details of the included studies and the extracted data can be found in Section 6.2, Tables 8 and 9.
The results of this rapid review have been categorised into common prognostic factors. These factors are demographic, ocular, lifestyle/behaviour, and systemic health related. The factors are then further categorised into specific prognostic factors or similar categories of prognostic factors.
As the scope of this prognostic factor review is broad, and the review conducted with exploratory aims, essential restrictions were put in place to make sure the review remained tenable within the limits of rapid review methodology. Included studies were therefore limited to a pre-determined list of countries (Section 5.1, Table 7) that were determined by the review team to have similar demographics and eye care systems to the UK. Studies were also included only if they had presented their findings as odds ratios, risk ratios/relative risk, or hazard ratios – an approach that is in line with other prognostic factor reviews (Riley et al. 2019) – and had used multivariate analyses to determine these. The use of multivariate analyses means, where an association has been identified, the reported prognostic factors have an effect on the outcome that is independent of the other factors controlled for. Factors controlled for in each study are included in Table 8; there was considerable variation in the types of factors and the number of factors controlled for in each study. Owing to this being a rapid review, it was not feasible to convert other types of outcomes into ratios as is sometimes done in prognostic factor reviews. This is discussed in the limitations of this review.
Using the Quality in Prognostic factor Studies (QUIPS) tool, all but one of the primary evidence sources were determined to be of low or moderate risk of bias across all six domains of the tool. Ten of the 17 studies were assessed as moderate risk of bias for prognostic factor or outcome measurement, with eight of these relying on self-reporting, leading to increased risk of recall bias. Similarly, there were concerns regarding loss to follow-up or study attrition in seven studies and it was unclear whether the strategy for model building was appropriate and based on a conceptual framework or model in four studies. One study (Barsam et al. 2017) was determined to be at high risk of bias due to its case-control design and only including a small number of the cases in multivariable modelling.
Using the Risk of Bias in Systematic reviews (ROBIS) tool, both systematic reviews included in this rapid review were deemed to have either low risk of bias (Kessel et al. 2015) or an unclear risk of bias (Dinu et al. 2019). For the systematic review deemed unclear, issues were centred around the failure to address heterogeneity, and a lack of clarity on whether subgroup analyses were pre-specified. Both studies included meta-analyses and the results of these were extracted for this rapid review. None of the identified primary evidence sources were included in either of the systematic reviews.
2.2 Demographic prognostic factors
Results for this section are summarised in Table 1 with comprehensive details available in Section 6.2, Tables 8 and 9.
2.2.1 Age
Nine identified studies examined the association of age with various ocular/vision conditions, including five prospective cohort analyses, one retrospective cohort analysis, one population-based longitudinal study, one cross-sectional study, and one case-control study. All of the included observational studies were of low to moderate risk of bias, with three studies rated as moderate due to some measures being self-reported and lack of clarity whether the strategy for multivariate model building was appropriate.
Only three studies reported on the same outcome, and found that aging is associated with an increased risk of developing open-angle glaucoma in adults aged 65 to 74 years, 55 to 84 years, and 55 years or over, respectively (Ekström 2012, Ekström & Hårleman 2023, Marcus et al. 2012). The two studies by Ekström were, however, identified by the review team as having a high risk of double reporting. Kang et al. (2012) found that increasing age is also a risk factor for exfoliation glaucoma or being an exfoliation glaucoma suspect. When compared to 40 to 55 year olds, the rate ratio increased for every 5-year bracket, with 55 to 60 year olds having approximately four times (rate ratio 4.33) the risk of developing exfoliation glaucoma or being a suspect case and those over 75 years old having approximately 46 times the risk (rate ratio 46.22).
Aging is also associated with increased odds of needing an eye care referral in adults over 50 years of age (Keel et al. 2017) or experiencing any kind of change in ocular status (Irving et al. 2016). For every one-year increase in age, the odds of having a change in ocular status increased by 3%.
Aging is associated with a reduced risk of experiencing a myopic change in refractive error at five years in adults aged 35 to 74 years, by 48% per year (Stingl et al. 2023). At the same time, it is associated with increased risk of experiencing a hyperopic change in refractive error over five years in adults aged 35 to 74 years, with 62% increased risk per year (Stingl et al. 2023).
Age was found not to be associated with the risk of progression of myopic maculopathy in high myopes (people with extreme or severe near-sightedness) aged between 35 and 74 (Hopf et al. 2022) or with developing visual field damage in glaucoma suspects of African or European descent (Khachatryan et al. 2015).
2.2.2 Sex
Eight studies were identified that examined the effect of sex as a prognostic factor for a change in ocular status. These included four prospective cohort studies, one retrospective cohort analysis, one longitudinal study, one cross-sectional study and one case-control study. All included studies were identified as having low to moderate risk of bias, with concerns around the use of self-reported measures in four studies.
Male sex was found to be a risk factor for requiring an eye care referral in adults over 50 years of age, with 24% higher odds than females (Keel et al. 2017). Males were also found to be at higher risk of developing open-angle glaucoma in adults aged 55 years and older, with 37% higher risk (Marcus et al. 2012). However, females are more likely to be diagnosed with exfoliation glaucoma or a suspect case of this, with males having less (32%) chance than females do (Kang et al. 2012). Females are also nearly 50% more likely than males to experience a myopic change in refractive error over five years in adults aged 35 to 74 years (Stingl et al. 2023).
Sex was not found to be associated with the risk of developing myopia in children (Guggenheim et al. 2012), or open-angle glaucoma in adults aged 55 to 84 years (Ekström & Hårleman 2023), progression of myopic maculopathy in high myopes aged 35 to 74 years (Hopf et al. 2022), or experiencing a change in ocular status (Irving et al. 2016).
2.2.3 Ethnicity/race
Two identified studies looked into the effect of ethnicity/race in relation to different eye conditions. This included a prospective cohort analysis and a retrospective cohort analysis. Both observational studies were judged to be at low risk of bias.
Glaucoma suspects, defined as eyes with a history of elevated intraocular pressure (IOP) and/or an optic disc appearance suspicious of glaucoma but normal visual fields at baseline in this study, of African descent were at higher risk of developing visual field damage than those of European descent if their mean IOP was 22 mmHg or higher with the hazard ratio increasing as IOP increased (Khachatryan et al. 2015). The study found that those with a mean IOP of 22 mmHg had double the risk of their European counterparts, whilst the risk was more than 3.5 times greater with a mean IOP of 26 mmHg. The study found that there was no significant association with race at IOPs of 10 to 20 mmHg.
Black ethnicity was also associated with increased risk of developing central retinal vein occlusion (CRVO) compared to White ethnicity in adults aged 55 years and over (hazard ratio 1.58 [95% confidence interval (CI) 1.25 to 1.99]) (Stem et al. 2013). Asian-American ethnicity was not deemed to be a risk factor according to this study.
2.2.4 Socioeconomic characteristics
Various socioeconomic factors were examined as potential prognostic factors in three identified studies. These were a prospective cohort study, a retrospective cohort study, and a cross-sectional study. All three studies were rated as low or low to moderate risk of bias.
Geographical remoteness and years of education were not found to be associated with the risk of eye care referral in adults over 50 years of age by Keel et al. (2017). This study was conducted in Australia and, thus there are concerns about the generalisability of this evidence to Wales due to much greater remoteness and distances to major urban settlements in Australia.
Education was found to not be associated with change in refractive error at five years in adults aged 35 to 74 years (Stingl et al. 2023). This same study also found that occupation is not associated with change in refractive error.
Lower household net worth was found to be associated with increased risk of developing CRVO in adults 55 years and older in an American study (Stem et al. 2013). Those with a household net worth of greater than US$500,000 had 27% lower risk of developing CRVO than those with a net worth less than US$25,000 (hazard ratio 0.73 [95% CI 0.56 to 0.96]).
2.2.5 Bottom line results for demographic prognostic factors
The evidence identifies suggests that age, sex, ethnicity, and household net worth are potential risk factors for changes in vision or ocular health. Aging and increasing age is associated with a general increased risk of change in ocular status, while sex, ethnicity and household net worth are dependent on the outcome examined. No studies were identified that examined the use of index of deprivation as a prognostic factor.
Across all studies in this review the certainty of the evidence is low due to the paucity of evidence for each outcome – with only one study identified in many cases. Though the evidence was deemed to be at low or moderate risk of bias, further research is necessary to inform any decision making in this area.
2.3 Ocular prognostic factors
Results for this section are summarised in Table 2 with comprehensive details available in Section 6.2, Tables 8 and 9.
2.3.1 Vision-related
Five identified studies looked at vision-related characteristics as prognostic factors for changes in ocular status. Four were prospective cohort studies and one was a case-control study. Three of the studies were rated as low to moderate risk of bias, with one (Barsam et al. 2017) deemed high risk of bias, due to the case-control study design meaning that the prognostic data was collected after the outcome was known and the low number of cases (21%) included in the multivariate model.
In a case-control study comparing people with keratoconus, a progressive condition causing thinning and irregular curvature of the cornea, who developed acute corneal hydrops (a sight-threatening complication of keratoconus that can leaving scarring) to those who did not, Barsam et al. (2017) found that worse visual acuity (VA) was associated with increased odds of developing corneal hydrops.
A prospective cohort study by Khachatryan et al. (2015) of glaucoma suspects found that a worse result on visual field assessment (mean deviation) at baseline was a risk factor for developing visual field damage (hazard ratio 1.04 (95% CI 1.02 to 1.06) per 0.1 dB decrease).
In a study by Stingl et al. (2023), baseline spherical equivalent refraction (SER) was found to be a risk factor for having a myopic shift in refractive error at five years in adults aged 35 to 74 years, with increasing myopia being a greater risk factor for a myopic shift (11% per dioptre more myopic). However, SER was not found to be associated with the risk of developing visual field damage in glaucoma suspects (Khachatryan et al. 2015) or for the progression of myopic maculopathy in high myopes aged 35 to 74 years (Hopf et al. 2022). High myopia was found to be associated with increased risk of incident open-angle glaucoma in adults aged 55 years and over (Marcus et al. 2012).
2.3.2 Ocular pathology
Four studies identified looked at various ocular pathologies as prognostic factors for other ocular pathology or changes in refractive error. This included one systematic review and meta-analysis, one prospective cohort analysis, one retrospective cohort analysis, and one case-control study. The meta-analysis was judged to have low concerns for risk of bias and the three observational studies were judged to be of low to moderate risk of bias, with two studies unclear whether the strategy for model building was appropriate.
Stem et al. (2013) investigated whether age-related macular degeneration (AMD), open-angle glaucoma, and cataract were prognostic factors for developing CRVO in adults of 55 years of age and older. They found that all three were associated with increased risk of developing CRVO with increased risks of 50%, 50% and 24% respectively compared to those without these conditions.
It was found that the presence of cataract is not associated with increased risk of a change in refractive error in adults aged 35 to 74 years (Stingl et al. 2023), and a meta-analysis of four studies found that undergoing cataract surgery was not associated with increased risk of progression to wet AMD in people with dry AMD 6 to 12 months after surgery (Kessel et al. 2015). Stingl et al. note that their findings are contrary to other cohort studies which report an association between nuclear cataract and a myopic shift in refractive error. They suggest this may be explained by the lack of differentiation of nuclear and cortical cataract in their study.
The presence of pseudoexfoliation was found not to be a risk factor for developing open-angle glaucoma in adults aged 55 to 84 years; odds ratio 1.27 (95% CI 0.63 to 2.57) (Ekström & Hårleman 2023). This is thought to be due to the strong interaction between increased IOP and the presence of pseudoexfoliation (see Section 2.3.3) and, therefore, pseudoexfoliation is not independently associated with increased risk of open-angle glaucoma.
2.3.3 Intraocular pressure
Five identified studies investigated IOP as a prognostic factor for ocular pathology or a change in refractive error. There were three prospective cohort analyses, one longitudinal study, and a case-control study. All studies were assessed as low to moderate risk of bias.
Ekström (2012) and Ekström & Hårleman (2023) confirmed that increasing IOP is associated with increased risk of open-angle glaucoma, something which is well established as stated in the studies. While pseudoexfoliation is not independently associated with glaucoma, mean IOP greater than or equal to 25 mmHg concurrent with pseudoexfoliation is associated with greater risk of incident open-angle glaucoma in 65 to 74 year olds (Ekström 2012).
A study of glaucoma suspects by Khachatryan et al. (2015) found that increasing IOP was not independently associated with increased risk of developing visual field damage in suspects of African or European descent; HR 0.97 per 1 mmHg increase (95% CI 0.92 to 1.03). However, as stated in Section 2.2, the risk of visual field damage in glaucoma suspects of African descent compared to European descent did show a positive correlation with mean IOP increase.
Hopf et al. (2022) found that increasing IOP increased the risk of progression of myopic maculopathy in high myopes aged 35 to 74 years by 62% per mmHg at 5 years. Whilst another study found that IOP is not associated with increased risk of a change in refractive error at 5 years in adults aged 35 to 74 years (Stingl et al. 2023).
2.3.4 Family history
Four studies were identified that investigated family history as a potential prognostic factor. These include two prospective cohort studies, a longitudinal study, and a case-control study. All three studies were judged as low to moderate risk of bias, with self-reporting of measures being a factor.
Three of the studies investigated positive family history of glaucoma as a risk factor for different types of glaucoma. Positive family history of glaucoma was found to be associated with over double (rate ratio 2.29) the risk of developing exfoliation glaucoma or becoming an exfoliation glaucoma suspect in adults (Kang et al. 2012). Positive history was associated with more than double (OR 2.24) the risk of developing open-angle glaucoma in adults aged 55 years and over in a study from The Netherlands (Marcus et al. 2012) and more than three times (OR 3.21) increased risk in adults aged 55 to 84 years (Ekström & Hårleman 2023).
Positive parental history of myopia was not associated with increased risk of children becoming myopic after age 11 years (Guggenheim et al. 2012). This was true for children with only one myopic parent or both parents.
2.3.5 Ocular parameters
Two prospective cohort studies were identified that examined other ocular parameters as potential prognostic factors. One study was rated as low risk of bias, whilst Kang et al. (2012) was rated low to moderate risk of bias due to self-reporting of both outcomes and prognostic factors.
It was found that central corneal thickness is not associated with risk of developing visual field damage in glaucoma suspects of African or European descent (Khachatryan et al. 2015). Eye colour was also found not to be associated with the risk of developing exfoliation glaucoma or becoming a exfoliation glaucoma suspect in adult men (Kang et al. 2012).
2.3.6 Bottom line results for ocular prognostic factors
The evidence identified shows that various ocular prognostic factors, which could be identified during a routine eye examination, were identified as risk factors for the development other ocular pathology or changes in vision or refractive error. This includes VA, visual field mean deviation, SER, various ocular pathologies, IOP, and family history of glaucoma.
As with Section 2.2, it is pertinent to note that the evidence summarised in this section is specific to the outcomes mentioned above, and cannot be extrapolated to cover all eye conditions. In many cases, a lack of evidence means that there is often only one study per prognostic factor / outcome pairing, and therefore the certainty of the evidence is low. There were two studies that reported positive family history of glaucoma as a risk factor for incident open-angle glaucoma and the confidence in this finding is also higher. Most included primary studies were of low or moderate risk of bias, with one at high risk of bias, whilst the included meta-analysis states that the studies it included were of moderate or very low quality.
2.4 Interval between eye examinations
Results for this section are summarised in Table 3 with comprehensive details available in Section 6.2, Tables 8 and 9.
Three of the identified studies investigated whether the length of time between eye examinations is a prognostic factor for changes in ocular health. This included two retrospective cohort analyses and a cross-sectional study. All three studies were of low or low to moderate risk of bias.
Keel et al. (2017) and Wright et al. (2020) examined whether increased time between eye examinations affected eye care referral rates and rates of referral to a general practitioner (GP), respectively. The odds of requiring an eye care referral increased 15% per year since last examination in the study by Keel et al. (2017) in adults aged 50 years and older. Delayed attendance at eye examinations was associated with 30% increased odds of requiring referral to a GP for 60 to 69 year olds and a 7% increase for those aged 70 years or over (Wright et al. 2020). Early attendance for an eye examination was associated with nearly three times increased odds of requiring GP referral in both age groups. However, this was believed to be due to early attendance usually being in response to the patient noticing symptomatic problems or because the optometrist recommended early assessment at the last examination.
The relationship between the time elapsed since previous eye examination and the odds of experiencing a change in ocular status (such as a change in vision or glasses prescription, emergence of new pathology, requiring a referral) was investigated by Irving et al. (2016). The study found that increasing the length of time elapsed between examinations is associated with an increased risk of experiencing a significant change in ocular status, with a 6% increase in risk per year.
2.4.1 Bottom line results for intervals between eye examinations
Increasing length of time between eye examinations is associated with increased risk of experiencing a change in ocular status, including requiring onward referral. The confidence in this finding is high as three studies reported this as a prognostic factor for similar outcomes. Due to the study designs of Keel et al. (2017) and Wright et al. (2020), it is possible that some of the participants in these studies were experiencing symptomatic eye issues.
2.5 Lifestyle/behaviour prognostic factors
Results for this section are summarised in Table 4 with comprehensive details available in Section 6.2, Tables 8 and 9.
2.5.1 Diet
Three of the identified studies investigated diet or alcohol intake as prognostic factors for changes in ocular status. This included one systematic review and meta-analysis, one prospective cohort study, and one longitudinal population-based cohort study. The two observational studies were rated as moderate risk of bias due to uncertainties around study attrition and some self-reporting of measures. The meta-analysis was rated as having unclear concerns of risk of bias due to heterogeneity in the studies not being addressed and a lack of clarity as to whether subgroup analyses were pre-specified.
In a meta-analysis of 26 studies, Dinu et al. (2019) found that higher meat intake is associated with higher risk of the occurrence or progression of early AMD, increasing the risk by 17%. Increasing alcohol intake was found to be associated with increased risk of all AMD and early AMD (20% and 29% increased risk respectively) but not with late AMD. Increased dietary intake of fish was found to have a protective effect against AMD with the risk of early AMD being reduced by 16%, late AMD by 21%, and all AMD by 18%. An increased intake of dairy products, plant products, and fats was not found to be associated with risk of AMD.
In a study on post-menopausal women, Elmore et al. (2022) found no association between dietary intake of fish or fatty acids and incident AMD. The study also investigated red blood cell fatty acid levels as a longer-term biomarker of fatty acid intake and still found no association between levels of any red blood cell polyunsaturated fatty acid levels and incident AMD.
Gopinath et al. (2014) investigated the effect of diet on the 5-year incidence of dual sensory impairment (concurrent visual and hearing impairment). The study found no association between having a higher total diet score (healthier diet) and the incidence of dual sensory impairment in adults aged over 49 years.
2.5.2 Smoking
One identified study investigated smoking as a prognostic factor. This was a prospective cohort study. The study was rated as low to moderate risk of bias due to issues with study attrition and lack of clarity on whether the model building strategy was appropriate.
Smoking is associated with increased risk of experiencing a hyperopic change in refractive error at five years in adults aged 35 to 74 years (Stingl et al. 2023), with the risk increasing by 31%. However, the study found that being an occasional smoker or former smoker does not increase the risk of having a hyperopic change in prescription compared to non-smokers.
2.5.3 Activity-related
Two studies were identified that investigated whether activity levels, or the types of activities done, are prognostic factors for refractive changes. One was a prospective cohort analysis and the other was a longitudinal study. Both observational studies were of low to moderate risk of bias, with study attrition being a common issue.
Guggenheim et al. (2012) examined the role of time spent outdoors and physical activity on myopia prevalence and progression. The study found that increased time spent outdoors was independently associated with lower risk of developing myopia after the age of 11 years, with the risk reducing by 35%. It also found that increased time spent reading was associated with a 32% increased risk of developing myopia after age 11, but that the amount of physical activity done/amount of sedentary time was not independently associated with the risk of developing myopia.
Stingl et al. (2023) also found that the amount of physical activity was not associated with increased risk of a change in refractive error at five years in adults aged 35 to 74 years.
2.5.4 Bottom line results for lifestyle/behaviour prognostic factors
Dietary intake of meat, fish, and alcohol are prognostic factors for incident AMD. However, there is discrepancy in the literature on the protective effect of fish intake in the sub-group of post-menopausal women.
Smoking is potentially a risk factor for hyperopic changes in refractive error. Increased time spent outdoors may protect against children developing myopia, whilst reading may be a risk factor for it. However, the amount of time being physically active does not appear to be associated with changes in refractive error.
As before, though all the studies included in this section of the rapid review are of moderate or low risk of bias, the findings are of low certainty due to the fact that there is generally only one study for each prognostic factor/outcome pairing. The findings therefore cannot be generalised beyond the outcome or specific populations that are presented in this section.
2.6 Systemic health prognostic factors
Results for this section are summarised in Table 5 with comprehensive details available in Section 6.2, Tables 8 and 9.
2.6.1 Cardiovascular/vascular issues
Five of the identified studies examined cardiovascular or vascular issues as prognostic factors for ocular changes. This included two prospective cohort studies, one retrospective cohort study, one cross-sectional study, and one case-control study. All the studies were of low or low to moderate risk of bias.
Treated hypertension was found not to be associated with increased risk of incident open-angle glaucoma in adults aged 55 to 84 years, however the effect of untreated hypertension was not investigated (Ekström & Hårleman 2023). However, increasing mean arterial pressure was associated with increased risk of visual field damage in glaucoma suspects of African or European descent, with a 3% increased risk per 1 mmHg (Khachatryan et al. 2015). Stem et al. (2013) found that hypertension is associated with increased risk of incident CRVO in adults aged 55 years and over. The risk increased by two-thirds compared to those without hypertension. Those with hypertension and high cholesterol still had increased risk of CRVO compared to those without these conditions but lower increased risk than hypertension alone (46% compared with 66%). Having hypertension, diabetes, and high cholesterol lead to CRVO risk increasing by 58%.
Peripheral arterial disease and hypercoagulable state were both found to be associated with higher risk of CRVO, increasing the risk 1.15 and 2.45 times respectively (Stem et al. 2013). Previous stroke was also associated with higher risk of CRVO (HR 1.44 [95% CI 1.23 to 1.68, p < 0.0001). However, self-reported previous stroke was not associated with higher risk of requiring eye care referral in adults aged 50 years or over (Keel et al. 2017).
Previous myocardial infarction was associated with a lower risk of incident CRVO in adults aged 50 years and over (Stem et al. 2013). The chance of developing CRVO was reduced by 28%; this may be due to treatments given after the myocardial infarction has happened. Ischaemic heart disease was also found to be associated with higher risk of incident open-angle glaucoma in adults aged 55 to 84 years, more than doubling the risk (Ekström & Hårleman 2023).
Stingl et al. (2023) found that a range of cardiovascular parameters were not associated with change in refractive error at five years in adults aged 35 to 74 years.
2.6.2 Diabetes
Two of the identified studies examined diabetes as a prognostic factor. These were a retrospective cohort analysis and a cross-sectional study. The retrospective cohort analysis was rated as low risk of bias, whilst the cross-sectional study was rated low to moderate risk due to self-reporting of some prognostic factors and only including covariates that were significant in univariate analysis in the multivariable model.
Having hypertension and diabetes was associated with higher risk of developing CRVO in adults aged 55 years and over, increasing the risk by 82% (Stem et al. 2013). As mentioned in Section 2.5.1, diabetes alongside hypertension and high cholesterol increased the risk of incident CRVO in this population by 58%.
Self-reported history of diabetes was not found to be associated with eye care referral rates in adults aged 50 years and over (Keel et al. 2017).
2.6.3 Women’s health
Two studies were identified that examined various aspects of women’s health/reproductive health as prognostic factors for eye conditions. Both were prospective cohort analyses. Fernández-Montero et al. (2017) was rated as moderate risk of bias due to self-reporting of outcomes and prognostic factors and due to the loss to follow-up rate. Pasquale & Kang (2011) was also rated as moderate risk for similar reasons.
Fernández-Montero et al. (2017) found that pregnancy was associated with lower risk of developing myopia or progression of existing myopia in women aged 20 to 50 years. This risk was decreased by 42% compared to women who were not pregnant and was proposed to be due to increased time spent outdoors during periods of maternity leave.
For women aged 40 and over, age at menarche was associated with increased risk of incident normal tension glaucoma (Pasquale & Kang 2011). Those with age at menarche older than 13 had 47% increased risk compared to those with age at menarche under 12 years. The length of time between menarche and menopause (reproductive duration) was not associated with risk of incident open-angle glaucoma.
Pasquale & Kang (2011) also found that oral contraceptive use was associated with the risk of incident open-angle glaucoma in women 40 years of age and over. Five years or greater use of oral contraceptives and time since discontinuing use of oral contraceptives less than 10 years were associated with increased risk of open-angle glaucoma. The risk was increased by 25% and 39% respectively compared to those who had never used oral contraceptives. Whether a woman had had children or not, and the number of children they have had, was not associated with incident open-angle glaucoma.
2.6.4 Other systemic health issues
In a case-control study examining risk factors for acute corneal hydrops in keratoconics, two atopic conditions were found to be associated with increased risk of developing corneal hydrops (Barsam et al. 2017). History of vernal conjunctivitis increased the risk by 15 times and asthma increased the risk by nearly five times. However, both had very wide 95% CI, suggesting these results are not very precise, and the multivariable model only included 15 cases and 144 controls out of the samples of 64 and 1794 respectively. This study was rated as high risk of bias due to the case-control design and the prognostic data being collected after the outcome was known and the low number of cases included in the multivariable model.
When investigating adults over 55 years of age, Marcus et al. (2012) found that use of any type of corticosteroid medications was not associated with increased risk of incident open-angle glaucoma. They acknowledged that this is contradictory to many other studies’ findings, but also noted studies with consistent findings that often found that corticosteroid use is associated with increased IOP but not necessarily with a diagnosis of glaucoma. This study was rated as moderate risk of bias due to a fairly low number of participants having follow-up data and some measures being self-reported.
2.6.5 Bottom line results for systemic health prognostic factors
There are many systemic health conditions that can be risk factors or protective factors for ocular pathology, refractive error, or the need for eye care referral. These include hypertension, high cholesterol, diabetes, heart disease, peripheral artery disease, stroke, hypercoagulable state, and atopy. However, this list is not exhaustive. Many of these were associated with CRVO.
Factors related to reproductive health, such as current pregnancy, use of oral contraceptives, and age at menarche, are also linked to glaucoma and myopia. Use of corticosteroids was not identified as a risk factor for glaucoma.
All findings for this section are of low certainty due to the lack of evidence available. Further research is necessary to understand the relationship between systemic health factors and visual health. These findings cannot be extrapolated beyond the outcomes or populations explored in this section.
3. DISCUSSION
3.1 Summary of the findings
The evidence included in this rapid review suggests that increasing age, sex, Black/African ethnicity, increasing IOP, positive family history of glaucoma, increasing length of time between eye examinations, hypertension, and heart disease are potential prognostic factors for a change in ocular health or vision. These were prognostic factors that were investigated in multiple studies; however, certainty in the evidence is low due to the majority of outcomes only being evidenced by one study. Similarly, the majority of studies were undertaken in specific populations, meaning that the association between these prognostic factors and the individual outcomes remains unclear in the general population. Single studies suggest that lower household net worth, worse VA, worse visual field mean deviation, SER, high myopia, AMD, glaucoma, cataract, diet, increasing alcohol intake, smoking, time spent outdoors, time spent reading, cholesterol, diabetes, peripheral arterial disease, hypercoagulable state, stroke, pregnancy, age at menarche, oral contraceptive use, and atopy are potential prognostic factors for a change in ocular status. This is summarised in Table 6.
Limited confidence in the results of this rapid review mean that these prognostic effects have limited applicability to the general population, owing to the specificity of the studies. Caution should therefore be taken when drawing from this rapid review, and further research is necessary to inform policy and practice.
It should also be noted that these findings are not specific to risk factors, with some studies also identifying protective factors. Each prognostic factor should be considered in relation to specific outcomes, rather than in relation to the overall category of a change in ocular status.
3.2 Strengths and limitations of the available evidence
One of the strengths of the available evidence is that all results were derived from multivariate analyses, presenting adjusting odds / risk / hazard ratios. This demonstrates that the prognostic factor of interest has an independent effect on the outcome. However, this is limited to only being independent of the other covariates included in the multivariate model, and these are not exhaustive. There is notable variation between studies in how many covariates they included in models, with some studies including as few as three covariates and others more than a dozen. Some studies did not clearly state what their adjustment factors were, or how they had decided which factors to include.
Limitations to the available evidence include only identifying two relevant studies that were carried out in the UK. Though search limits and eligibility criteria were applied to ensure only evidence from countries sufficiently similar to the UK were included in the review, the generalisability of any of these studies to Wales remains uncertain. Sample sizes of the studies also varied considerably with some being quite small, only several hundred participants. The sample populations were also often quite specific, such as post-menopausal women, female graduates, or glaucoma suspects, meaning that it is difficult or not possible to apply these findings to the broader population. There was comparatively less evidence identified that examined prognostic factors for conditions that would not require onward referral and could be managed by an optometrist, potentially influencing their decision on frequency of eye examinations, than conditions that would be referred to be managed by other health professionals.
There was a lack of relevant systematic reviews and meta-analyses identified for this review, which would have helped increase the certainty of the evidence by collating more studies. There were also no RCTs identified. However, the types of primary evidence included in the review were of appropriate design for a prognostic factor review. Observational studies, such as cohort studies and case-control studies, can be useful to these types of review and variation in study designs is to be expected (Riley et al. 2019). The included studies were of reasonable quality, with risk of bias ranging from low to moderate as judged using the QUIPS and ROBIS tools. Only one primary study was rated as high risk of bias. However, the data in a number of studies were subject to bias as it was self-reported from participants or their carers. Questionnaires were used in several studies to collect both prognostic and outcome data, and this may lead to high risk of recall bias.
Finally, there was a distinct lack of evidence identified in children and younger adults. Only three studies included children in their study population, and only one of these reported results specifically for children. Similarly, only a small number of studies included adults aged 18-39 years and no studies reported specifically on younger adults. Further research is needed in these populations.
3.3 Strengths and limitations of this Rapid Review
This rapid review was strictly limited to the included studies that were deemed to align with the research question and protocol, the scope of which was broad owing to the exploratory nature of this review. Controls intended to manage the amount of retrieved evidence were used, such as strict exclusion criteria and date limits and as such the methods used in this rapid review have been robust and pragmatic. However, it is crucial to note that due to the nature of rapid review methodology there remains the possibility that additional relevant studies were not identified. Additionally, some identified studies that reported findings relevant to the review question were excluded due to not reporting multivariate results or because the findings were not presented as odds/hazard/risk ratios. Sometimes these results can be converted to ratios, however, due to the nature of rapid review, it was not feasible to conduct this and include these studies. As such, the review team were reliant on interpreting the results of studies that have differing levels of quality and their own limitations. This therefore impacts the confidence of this review’s conclusions.
3.4 Implications for policy and practice
The low certainty of the evidence in this review means caution should be taken should this review be used for decision making on appropriate eye examination intervals. Additionally, there is very little data from the UK and, thus, the generalisability of the findings to the Welsh population is uncertain.
This review should be used to identify what are thought to be the key prognostic factors and patient characteristics that could be used when an optometrist is determining an individual patient’s risk of a change in ocular status, and therefore the appropriate interval until their next eye examination and suggesting these for further targeted research and evidence synthesis. The chosen factors or characteristics should be specific and narrow in scope, so that the limitations discussed above are mitigated. Alternatively, further research could be conducted looking at prognostic factors for specific ocular outcomes instead. The implications for future research are discussed in more detail below.
3.5 Implications for future research
Any further research undertaken to inform guidance on appropriate eye examination re-assessment intervals should be much narrower in focus to ensure as much relevant and useful evidence as possible is gathered. Prognostic factors or specific ocular conditions of interest potentially need to be investigated individually for their effect on a change in ocular status.
This rapid review focused on incident conditions or progression of existing conditions. Prevalence data and prognostic factors for prevalent eye conditions or vision problems may also be useful for decision makers producing guidance on eye examination intervals and further evidence review could be performed in this area.
It has been noted in previous evidence-based guidelines on eye examination frequency that there is a lack of data in younger adults aged under 40 years (Robinson et al. 2012). This was also found to be the case during this review. Therefore, further research is required in this demographic. This is a demographic that is assumed to be at lower risk of ocular issues, but published evidence is lacking to support this claim and research should be conducted to determine if this is the case.
This review has identified a significant lack of evidence that would be needed to make confident conclusions to the research question and represents the findings of evidence that may not be generalisable to Wales, limiting the validity of this review’s conclusions. More high-quality research must be undertaken in the populations of interest in order to inform and guide policy.
3.6 Economic considerations*
Sight loss costs the UK economy £25 billion per annum (RNIB 2021).
Over 2 million people in the UK are currently living with sight loss (NHS 2021).
The economic implications of appropriate or inappropriate testing intervals for different causes of vision loss will be different.
A new case of age-related macular degeneration (AMD) in an adult aged 50 or over, costs the UK economy £73,350 over the person’s lifetime. Lifetime costs to the UK economy for a person diagnosed with glaucoma are approximately £49,800 per person. Reducing the prevalence of these conditions by just 14 or 20 cases respectively could save the UK economy £1 million in lifetime costs (Fight for Sight 2020).
On economic grounds, early detection of AMD in eye care services and the eye care pathway may be of benefit due to the level of prevalence and associated long term costs to the NHS as the condition causes irreversible, life limiting damage (Stahl 2020, Pezzullo et al. 2018).
Draft National Institute for Health and Care Excellence (NICE) Guidance for Diabetic Retinopathy (DR) examinations suggest the use of ultrawide-field imaging for diagnosing and monitoring progression. The new guidance publishes in early 2024. DR costs the UK economy £80 million per annum when adjusted to October 2023 prices** (Hex et al. 2012).
The earlier detection of eye conditions through regular screening can identify conditions before severely impactful symptoms manifest. When captured at a population wide scale, this can result in significant economic savings (Fight for Sight 2020).
*This section has been completed by the Centre for Health Economics & Medicines Evaluation (CHEME), Bangor University.
** Prices adjusted using Bank of England Inflation Calculator.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
5. RAPID REVIEW METHODS
5.1 Eligibility criteria
Definitions: Refractive error – A common eye disorder when the eye does not clearly focus images, which can usually be corrected by spectacles or contact lenses. The most common types of refractive error are myopia (shortsightedness), hypermetropia/hyperopia (longsightedness), astigmatism and presbyopia (reduced ability to focus on near objects); Visual acuity – A person’s ability to recognise small details with precision, also referred to as clarity of vision.
5.2 Literature search
Prior to planning this review, a preliminary search for existing reviews was undertaken of Cochrane Database of Systematic Reviews, NIHR Journals Library, Trip database, KSR Evidence, Canadian Agency for Drugs and Technologies in Health, Prospero, PubMed, NICE, SIGN, Epistemonikos, Google Advanced Search, and Google Scholar using the keywords sight test, eye examination, eye test, sight examination, routine, frequency, interval, recall, and time. The findings were presented to the stakeholders and used to refine the scope of the present rapid review, and to inform the methods.
A comprehensive search was conducted to identify any additional English-language reviews from 2009 onwards. An analysis of the text words contained in the title and abstracts, and of the index terms used to describe any relevant reviews already identified were used to inform the search. The full search strategy was designed and run using Ovid Medline and then translated to all other databases:
CINAHL via the EBSCO platform
Embase via the Ovid platform
Cochrane Library database
Epistemonikos
This was followed by a thorough search for relevant English-language primary studies from 2009 onwards on the following databases:
CINAHL via the EBSCO platform
Medline and Embase via the Ovid platform
The full searches for English-language reviews and primary studies can be found in Appendix 1.
Grey literature sources, including websites of key third sector and government organisations, identified by the review team, or provided by Stakeholders were also searched (see Appendix 2).
5.3 Reference management
All citations retrieved from the database searches were imported or entered manually into EndNoteTM (Thomson Reuters, CA, USA) and duplicates removed by a single reviewer. The citations that remained were exported as a TXT file and imported to RayyanTM for study selection. Grey literature search results were added to an Excel spreadsheet and cross-checked against the database search results.
5.4 Study selection process
Two reviewers screened 20% of titles and abstracts independently. If 20% is equal to less than 200 total records, then the two reviewers will screen 200 records. After this, the level of agreement was assessed with disagreements settled by discussion and consensus. Both reviewers had to achieve at least 80% agreement on screened records before progressing to the next stage. The remaining titles and abstracts were screened by the primary reviewer alone. 20% of full texts were screened by both reviewers, with the same agreement threshold (80%) as before necessary before the remaining records could be screened by the primary reviewer alone. During independent screening, the primary reviewer consulted with the secondary reviewer in the case of any uncertainties.
5.5 Data extraction
Data extraction was based on the outlined eligibility criteria. We extracted details/characteristics on study country, study design, number of participants, relevant outcomes (see eligibility criteria) and study settings. The Checklist for Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies (CHARMS-PF) (Riley et al. 2019) was used to guide data extraction.
Data extraction was completed by individual reviewers and checked by a second reviewer (see Section 6.2 for completed data extraction forms for all included studies). In line with other prognostic factor reviews, data were only extracted from studies that reported prognostic factors as hazard ratios, odds ratios, or risk ratios/relative risk. Only multivariate or adjusted ratios were extracted so that only factors that were independently associated with outcomes were included in the report. Studies were excluded if they only reported unadjusted/univariate results. Relevant prevalence or condition progression rates were also extracted from studies that had reported the ratios listed above.
5.6 Quality appraisal
Study quality was assessed using the Risk of Bias in Systematic Reviews (ROBIS) tool (Whiting et al. 2016) for included systematic reviews and using the Quality in Prognostic Factor Studies (QUIPS) tool for included primary studies (Hayden et al. 2013). Critical appraisal was completed by individual reviewers and checked by a second reviewer. Studies of all quality were included.
5.7 Synthesis
We undertook narrative synthesis of the evidence identified based on the selection criteria outlined above.
5.8 Assessment of body of evidence
All evidence selected after the sift stage was deemed fit for inclusion in the final review. Due to the scope of this review and the methodological constraints of rapid review, formal assessment of the body of evidence using GRADE was not feasible in this case. An informal assessment of the evidence has been conducted.
6. EVIDENCE


6.2 Data extraction
All of the studies included in the rapid review are listed here. This includes two systematic reviews (Table 8) and 17 primary studies (Table 9).
6.3 Quality appraisal
6.4 Information available on request
The protocol, search strategies, and excluded studies for this rapid review are available on request.
7. ADDITIONAL INFORMATION
7.1 Conflicts of interest
The authors declare they have no conflicts of interest to report.
7.2 Acknowledgements
The authors would like to thank Rebecca Bartlett, Mike George, David O’Sullivan, Sarah O’Sullivan-Adams, Tim Morgan, Robert Hall and Rashmi Kumar for their contributions during stakeholder meetings in guiding the focus of the review and interpretation of findings.
8. APPENDIX
APPENDIX 1: Search Strategies
Searches for Secondary Research Medline Search Strategy
Ovid MEDLINE(R) ALL <1946 to August 03, 2023>
Conducted 03.08.2023
EMBASE Search Strategy
Conducted 03.08.2023
CINAHL Search Strategy
Conducted 03.08.2023
Epistemonikos
Searches for Primary Research Medline Search Strategy
Ovid MEDLINE(R) ALL <1946 to August 21, 2023>
Conducted 21.08.2023
EMBASE Search Strategy
Conducted 21.08.2023
CINAHL Search Strategy
Conducted 21.08.2023
APPENDIX 2: Grey Literature resources
Abbreviations
- AMD
- Age-related macular degeneration
- CI
- Confidence interval
- CRVO
- Central retinal vein occlusion
- HR
- Hazard ratio
- IOP
- Intraocular pressure
- OR
- Odds ratio
- QUIPS
- Quality in Prognostic factor Studies
- RCT
- Randomised controlled trial
- ROBIS
- Risk of Bias in Systematic reviews
- RR
- Risk ratio / relative risk
- SER
- Spherical equivalent refraction
- VA
- Visual acuity





{kind=link}
{kind=link}