
ABSTRACT
Anti-obesity medications (AOMs) are used with lifestyle change support for weight management for adults with obesity. We investigated whether initiation of AOMs appeared to reduce attempted lifestyle changes. We searched for orlistat, liraglutide, semaglutide, and low-fat reducing diet (LFRD) trials in a trial register, Medline, Embase and systematic reviews from 1990 to June 2023. Weight changes in placebo groups of AOM trials with lifestyle interventions were compared to weight changes in LFRD trials. 16 orlistat, 7 liraglutide, 5 semaglutide, and 7 LFRD trials were included. Weight loss in orlistat placebo groups was 1.1kg less than LFRDs, a statistically non-significant difference, where last observation carried forward values were used for missing data in trials. Adjustment with baseline observation carried forward found 2.6kg less weight lost, a significant difference. Last observation carried forward data for orlistat trials providing completer data found a 0.2kg difference.
Liraglutide placebo groups had 2.1kg less weight lost than predicted from LFRD trials. Semaglutide placebo groups had 2.0kg less weight loss.
Compensatory reductions in changes to lifestyle behaviours may result following AOM initiation, but this needs to be explored further. Variability in trial design and study populations may contribute to the differences in weight change found.
INTRODUCTION
Adults with obesity are supported to lose weight through changing diet and physical activity (PA) with behavioural interventions1,2. Where the target weight is not achieved or maintained, additional support can be provided through the initiation of anti-obesity medications (AOMs) 1. Currently, several AOMs have been approved for use by pharmaceutical regulatory agencies, including orlistat3–5, liraglutide6–8 and semaglutide9–11. Orlistat is a lipase inhibitor, blocking the function of gastrointestinal lipases and thus blocking the absorption of fat3–5. Liraglutide and semaglutide are both glucagon-like peptide-1 (GLP-1) agonists, also used by people with type 2 diabetes, which work by increasing insulin release and inhibiting glucagon release. However, GLP-1 agonists have also been found to delay gastric emptying and reduce appetite via central control, hence, assisting with weight loss7,8,10–12.
AOMs should be prescribed alongside a reduced calorie diet and modifications to PA, where possible, to maximise weight loss¹, meaning initiation of AOMs may promote healthy behaviours. It has, however, been suggested that compensatory behaviours may occur, with users tending to substitute a healthy lifestyle for taking a drug13,14. There are currently no studies assessing evidence of compensatory behaviours following AOM initiation. However, a recent scoping review15 looked for a relationship between initiation of lipid lowering drugs (LLD) and/or anti-hypertensive drugs and healthy diet in observational literature. Like AOMs, it is recommended that users of LLDs and anti-hypertensive drugs use them in addition to lifestyle changes to lower their cardiovascular disease risk factors further16,17. The review found that in 9 of the 17 included studies, use of LLDs or anti-hypertensive drugs was not always associated with improvements in diet15, suggesting lifestyle modification advice was either not received or was not acted upon by individuals starting these drugs. Similarly, a cohort study carried out between 2000 and 2013 on lifestyle behaviours following the initiation of anti-hypertensives and statins18 found initiators of the medications had a larger increase in BMI (difference of 0.19kg/m²) and were more likely to reduce PA (difference of −0.09 hours/day) compared with non-initiators. However, initiation did result in a reduction in alcohol consumption and higher likelihood of stopping smoking. It is possible that this increase in BMI resulted from replacing a healthier lifestyle with medication use. However, smoking cessation is associated with subsequent weight gain that cannot be reduced by PA alone19. Regardless, initiators may still be less healthy than their non-initiator counterparts. Statin use is associated with muscle complaints20 which might make it more difficult for some initiators to take part in PA18.
In 2005, Esposito and Giugliano13 commented on placebo participants limited weight loss during a randomised controlled trial (RCT) for a now unavailable AOM, rimonabant, implying they did not follow the prescribed dietary deficit of 600 kcal/d. In response, Brown and Avenell14 added that similar limited weight loss can be seen in placebo groups of orlistat RCTs. It was suggested that the participants of drug RCTs do not follow the dietary advice provided to participants to the same degree as those in dietary intervention RCTs, however, it was recognised that the higher BMI in participants of AOM RCTs may mean they may have an element of treatment resistance. More recently, Willet also described issues regarding behavioural compensation following initiation of AOMs21. A comparison of weight loss seen in AOM trials compared with non-drug diet trials is therefore warranted to see if this effect is present.
METHODS
The search strategy, study eligibility criteria and statistical approaches of this systematic review were predefined in an unpublished research protocol.
Study selection
Included trials were RCTs with a weight loss intervention for adults (age ≥18 years) with obesity (mean body mass index (BMI) at baseline ≥30kg/m²) with follow-up of at least 12 months (68 weeks for semaglutide) from randomisation. Interventions included were (1) orlistat dose of 120mg three times daily, (2) liraglutide dose 3.0mg subcutaneously once daily, (3) semaglutide dose 2.4mg subcutaneously once weekly or (4) low-fat reducing diet (LFRD) advice. Drug RCTs were compared to placebo. Included drug trials included advice on hypocaloric diets to all trial groups, but did not include those with meal replacements. For orlistat RCTs, advice regarding a LFRD (stating low-fat and/or less than 30% of dietary intake from fat), as per orlistat prescribing guidance3, must have been provided to all participants. LFRD intervention RCTs were compared with no or minimal intervention and did not describe providing physical activity (PA) advice, allowing for comparison of weight change to orlistat RCTs where PA advice was often not described.
Literature search
The reference list of a systematic review on the efficacy of anti-obesity medications 22 (last date of search strategy March 23, 2021) was searched for relevant orlistat, liraglutide and semaglutide RCTs. Additionally, a database search of Medline (Ovid) and Embase (Ovid) for drug weight loss RCTs from 1990 to present (January 06, 2023 for orlistat; June 19, 2023 for liraglutide; June 20, 2023 for semaglutide) was carried out.
A rapid search of the reference lists of previous systematic reviews23–25 was conducted for LFRD RCTs. Additionally, a database search of the University of Aberdeen Health Services Research Unit’s obesity trials’ register for low-fat weight loss trials was undertaken on January 13, 2023. This database, of all adult weight loss trials with a follow-up of at least one year, contains relevant searches of Medline, Embase and the Cochrane Register of RCTs and had been continuously updated from 1966 until 2017. Finally, a brief database search for LFRD RCTs from 2017 to January 2023 using search strategy for RCT and obesity and low fat.tw or low-fat.tw was completed. Duplicates were removed, and titles and abstracts were screened and excluded if not relevant. Full texts were independently analysed by two authors (AA and MM) to produce the final list of included weight loss trials.
Data extraction
Data were extracted regarding the (1) inclusion and exclusion criteria of each trial, (2) location of the study, (3) source of funding, (4) run-in period, (5) the number of contacts during the first year of the study, (6) advice given and (7) by whom, and (8) the methods of statistical analysis. The baseline characteristics of participants, including (a) mean age, (b) sex, (c) mean BMI, (d) co-morbidities, (e) ethnicity, and (f) socioeconomic status were also extracted. Data were extracted by MM and verified by AA with differences resolved through discussion.
For orlistat and LFRD RCTs, the mean weight change in kilograms (kg) and standard deviation (SD) at 12 months were extracted. Last observation carried forward (LOCF) data were used when provided if no other data for all participants randomised were available. Where trials also provided separate data for completers only, this was extracted and analysed separately.
Most liraglutide RCTs presented weight change as a percentage at 12 months and, as such, data were extracted and analysed in this form. Semaglutide RCTs also presented weight change as percentage change at 68 weeks and these data were extracted for analysis. Few liraglutide and semaglutide trials presented measures of variability and it was decided these values would not be estimated, thus meta-analysis was not possible for these trials. The weighted mean for percentage weight change for these trials was therefore calculated and used to estimate weight change in kg. Where data were presented in a different format to those required, relevant formulae were used as previously described elsewhere24.
Data for the number of participants randomised and the number of completers (on-drug) were extracted to calculate the number of dropouts. Where the number of completers at 12 months (68 weeks for semaglutide) was not stated, the number of completers at the end of the study was used. Where there were several intervention arms, dropouts for relevant arms were combined by addition of data.
Data analysis and reporting
Meta-analysis was used to analyse pooled data, involving comparison groups from included studies. Orlistat intervention groups were compared to placebo groups and LFRD intervention groups were compared to control. Review manager version 5.426 was used to conduct meta-analyses to compare interventions. For weight, a random-effects model was used since high heterogeneity between trials was expected. Data were analysed at 12 months to allow a common follow-up time. This was also the most common follow-up time, allowing for maximal data for comparison. A continuous inverse variance method was used to calculate the mean difference for weight change data and a dichotomous inverse variance method was used to calculate the mean difference for dropout data. A dichotomous Mantel-Haenszel method was used to calculate the risk ratio (RR). Heterogeneity was tested using the I² statistic with an I² value greater than 50% suggesting moderate heterogeneity27.
To assess the effect AOM initiation has on lifestyle behaviours, the pooled mean of the weight changes in the placebo groups in orlistat, liraglutide, and semaglutide RCTS were compared to the mean difference in weight change between the LFRD groups and control.
Statistical methods for analysis of weight differences - the pooled mean, pooled variance, and confidence intervals (CI) for the orlistat and placebo groups were calculated to allow for comparison to the LFRD RCTs. The pooled mean and variance were calculated using the respective formulae  , and
, and  , where:
, where:
ni are the number of observations in trial i receiving the respective treatment
x^i is the mean weight change in trial i for the respective treatment
S2i is the variance in trial i for the respective treatment
k are the number of trials of the respective treatment
The confidence interval for the two groups is obtained as xp ±1.96 √s2p/np where: the total number of observations, np = Σki=1 ni
The meta-analysis mean difference was used to obtain the estimated effect size for the LFRD with the standard error estimated by the difference in the upper and lower limits of the confidence interval divided by 3.92. These were then compared using a two sample independent t-test to the mean and standard deviation obtained from the pooled means and variances of the respective orlistat and placebo trials to make a formal statistical comparison.
Baseline observation carried forward adjustments – a post hoc adjustment of weight data from LOCF to baseline observation carried forward (BOCF) for participants that dropped out of the orlistat trials was completed for trials that reported separate data for completers. The method for this adjustment is described elsewhere28.
RESULTS
Search results
Figure S1 in the online supplement presents the study selection flow diagram.
Study characteristics
The descriptions of drug studies included in this review are summarised in the Table S1 in the supplement. 12/16 orlistat RCTs, 1/7 liraglutide RCTs and 0/5 semaglutide RCTs described a run-in period prior to randomisation. 10/16 orlistat RCTs, 7/7 liraglutide RCTs and 5/5 semaglutide RCTs reported giving advice regarding PA to participants. No RCTs provided a PA programme for participants to attend. The number of contacts by 12 months (68 weeks for semaglutide) ranged from 11 to 20 in orlistat RCTs, 12 to 23 in liraglutide RCTs and 12 to 21 in semaglutide RCTs. 8/16 orlistat RCTs, 7/7 liraglutide RCTs, and 5/5 semaglutide RCTs reported the advice and counselling received by participants was from a dietician or similarly qualified healthcare professional.
The descriptions of each included LFRD RCT are summarised in the Table S2 in the supplement. LFRD RCTs did not describe run-in periods prior to randomisation or describe providing PA advice to participants. Participants in the control groups were told to not change their dietary or PA patterns, other than one RCT29 where the control group were told to try to lose weight, however, they were given no formal counselling. The number of contacts by 12 months of the studies ranged from 4 to 32. Where details regarding who provided counselling advice were reported, RCTs had registered dieticians providing counselling.
The baseline characteristics of the participants of each drug RCT included in this review are summarised in the Table S3 in the supplement. The age ranges of participants at baseline were similar between the drug RCTs. All drug RCTs tended to recruit more female than male participants. Participants in orlistat RCTs (means 33kg/m²-38kg/m²) tended to have a lower mean baseline BMI compared to participants in liraglutide RCTs (means 35kg/m²-40kg/m²) and semaglutide RCTs (means 36kg/m²-39kg/m² apart from one RCT30 where only participants of Asian ethnic origin were included, and the mean baseline BMI was 32kg/m²). 8/16 of orlistat RCTs, 4/7 liraglutide RCTs and 5/5 semaglutide RCTs recruited participants due to their co-morbidities. Where details regarding the ethnicity of participants were provided, the majority of participants in each RCT were white. Details regarding the socioeconomic status of participants were not provided in any of the drug RCTs.
The baseline characteristics of participants in LFRD RCTs are summarised in Table S4 in the supplement. The age ranges of participants were similar to those in the drug RCTs. 3/7 RCTs included more female than male participants, with one of those trials including only female participants. The mean baseline BMI ranged from 29 kg/m² to 35 kg/m². The BMI for the RCT31 with BMI below 30kg/m² was for completers of the intervention, not for those randomised. It was therefore presumed that the BMI of participants randomised would be ≥30kg/m² and therefore included in this review. 5/7 RCTs recruited participants due to their co-morbidities. Where details regarding the ethnicity of participants were provided, the majority of participants in each RCT were white. Only one RCT reported on the socioeconomic status of participants.
All drug RCTs were sponsored by the drug manufacturer: orlistat RCTs were sponsored by Roche, and both liraglutide and semaglutide RCTs were sponsored by Novo Nordisk. One LFRD RCT29 was funded by Astra-Merck. Another LFRD RCT32 was funded by the insurance company “Vital Friskvern”. The remaining LFRD RCTs were not funded by commercial companies.
Weight change
Orlistat: all included RCTs
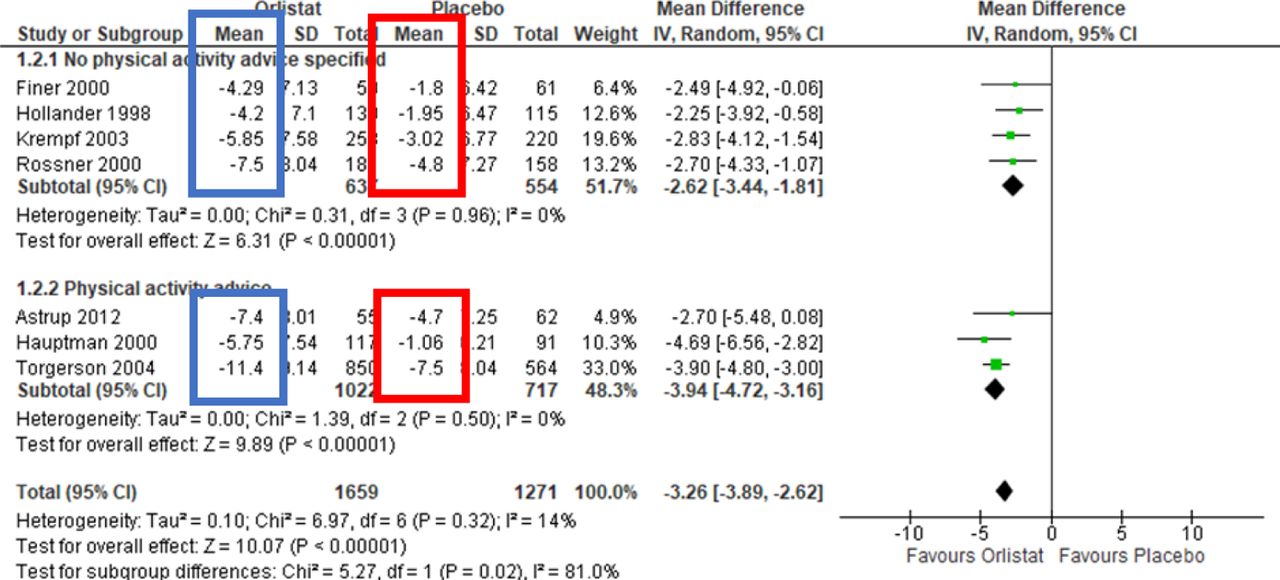
The mean weight reductions in those randomised to the orlistat intervention groups were always larger than those in the placebo groups. All placebo groups lost weight. Figure 1 shows the forest plot for meta-analysis of orlistat RCTs included 10,181 participants in which data for weight change at 12 months were available. The mean difference [95%CI] for weight change between the orlistat intervention groups and the placebo/control groups was −3.0kg [-3.5, −2.6]. Heterogeneity between the studies was 63% suggesting moderate heterogeneity between the trials.
The weighted mean weight change was calculated individually for the orlistat groups and the placebo groups. For the orlistat intervention group, the mean [95%CI] weight change was −7.0kg [-7.2, −6.8] (Figure 1, blue boxes). The mean [95%CI] weight change in the placebo group was −3.7kg [-3.8, −3.5] (Figure 1, red boxes).

Mean difference weight change in kg for all orlistat trials versus placebo
LFRD
The mean weight reductions were always larger in the LFRD groups than the control. Figure 2 shows the forest plot for meta-analysis of LFRD RCTs included 1,008 participants in which data at 12 months were available. The mean difference [95%CI] for weight change between the LFRD groups and the control groups was −4.8kg [-6.2, −3.4]. Heterogeneity between the studies was 69% suggesting moderate heterogeneity between the trials.

Mean difference weight change in kg for all LFRD trials versus control
Liraglutide
Table 1 shows the weight change (%) of those randomised in liraglutide RCTs. Those randomised to liraglutide always had a larger weight change than those randomised to placebo. The weighted mean weight changes for 3,511 participants randomised to liraglutide 3mg per day and 2,093 participants randomised to placebo in the liraglutide RCTs were calculated. Those randomised to liraglutide lost, on average, 7.8% of their initial body weight. Those randomised to placebo lost, on average, 2.5% of their initial body weight. When the weighted average baseline weight was calculated and used to calculate weight change in kg, those randomised to liraglutide lost an estimated 8.2kg compared to those randomised to placebo who lost an estimated 2.7kg.
Semaglutide
Table 2 shows the weight change (%) of those randomised in semaglutide RCTs. Those randomised to semaglutide always had a larger weight change than those randomised to placebo The weighted mean weight changes for 2,136 participants randomised to semaglutide 2.4mg per week and 1,333 participants randomised to placebo in the semaglutide RCTs were calculated. Those randomised to semaglutide lost, on average, 13.9% of their initial body weight. Those randomised to placebo lost, on average, 2.7% of their initial body weight. When the weighted average baseline weight was calculated and used to calculate weight change in kg, those randomised to semaglutide lost an estimated 14.3kg, compared to those randomised to placebo who lost an estimated 2.8kg.
Attrition
Orlistat
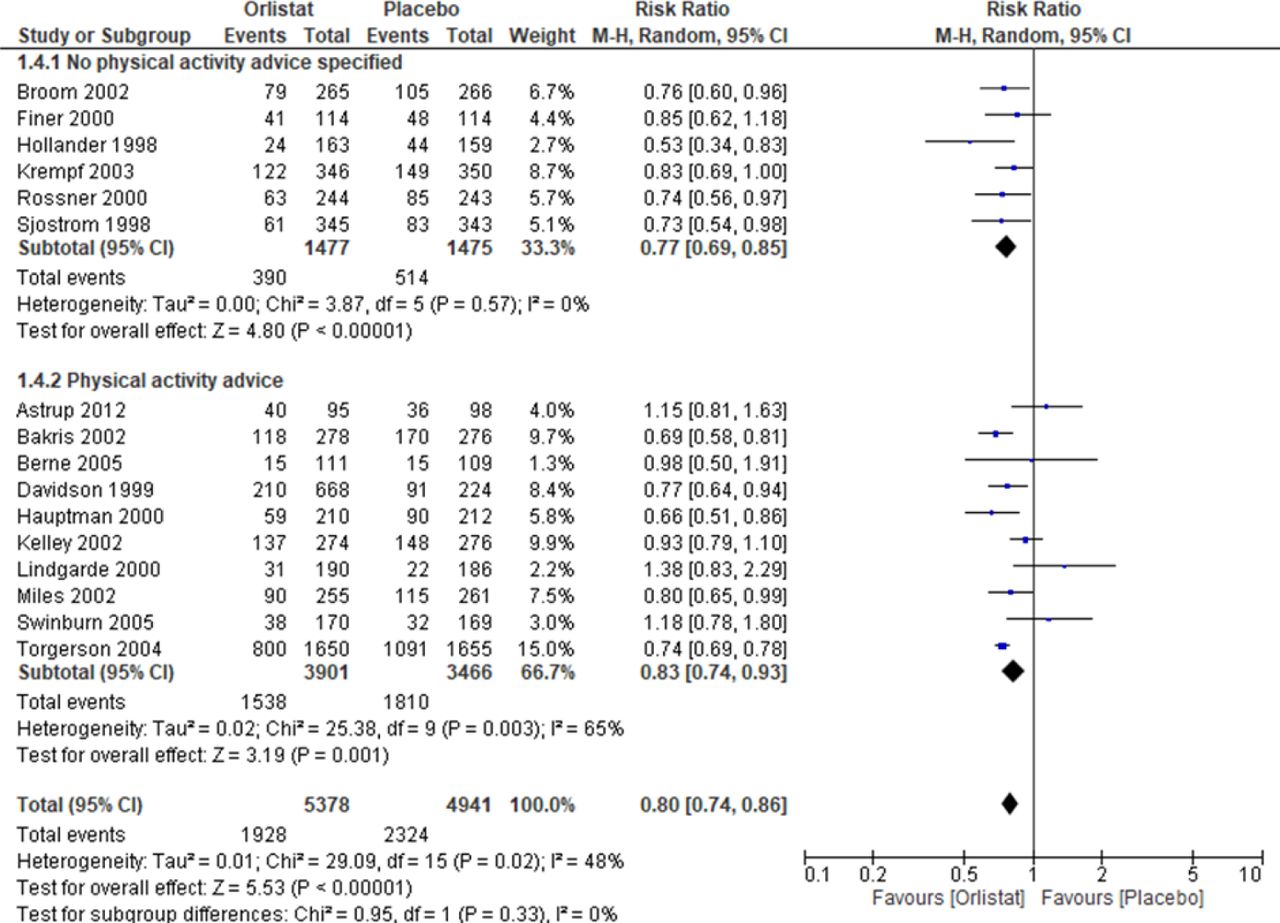
Orlistat RCTs experienced significant numbers of dropouts throughout the trials. Meta-analysis of orlistat trials included 10,319 participants in which dropout data were available (Figure S2 in the supplement). The risk ratio [95%CI] for dropouts between the orlistat intervention groups and the
placebo groups was 0.8 [0.7, 0.9]. Participants randomised to the placebo group were more likely to drop out than the orlistat participants.
LFRD
Meta-analysis of LFRD RCTs included 911 participants in which dropout data were available (Figure S3 in the supplement). The risk ratio [95%CI] for dropouts between the LFRD groups and the control groups was 1.4 [1.1, 1.9]. Participants randomised to the LFRD group were more likely to drop out than the control participants.
Liraglutide
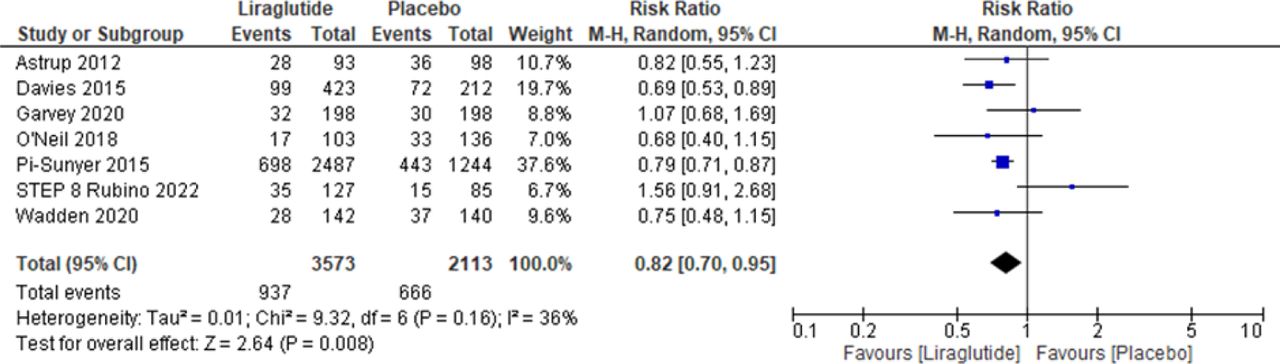
Meta-analysis of liraglutide RCTs included 5,686 participants in which dropout data were available (Figure S4 in the supplement). The risk ratio [95%CI] for dropouts between the liraglutide groups and the placebo groups was 0.8 [0.7, 1.0]. Those randomised to placebo were more likely to drop out than those randomised to liraglutide intervention.
Semaglutide
Meta-analysis of semaglutide RCTs included 3,583 participants in which dropout data were available (Figure S5 in the supplement). The risk ratio [95%CI] for dropouts between the semaglutide groups and the placebo groups was 0.8 [0.6, 1.0]. Those randomised to placebo were more likely to drop out than those randomised to semaglutide intervention.
Adjustment to baseline observation carried forward (BOCF) for orlistat RCTs: trials presenting both completers and LOCF data
Orlistat trials that included data for completers only found a mean difference [95%CI] for weight change between the orlistat intervention groups and the placebo groups to be −3.3kg [-3.9, −2.6] (Figure 3). Following adjustments to BOCF for those who dropped out in these RCTs, the orlistat intervention groups had a mean [95%CI] weight change of −5.0kg [-5.4, −4.7] at 12 months. The mean [95%CI] weight change in the placebo group was −2.2kg [-2.5, −1.9].

Mean difference weight change in kg for all orlistat trials versus placebo (completers only)
Where these trials only were analysed but using the original LOCF data, a mean difference [95%CI] for weight change between orlistat and placebo groups of −3.0kg [-3.9, −2.2] was found. The orlistat intervention groups had a mean [95%CI] weight change of −8.2kg [-8.5, −7.9]. The mean [95%CI] weight change in the placebo group was −4.6kg [-4.8, −4.3] (Figure S6 in the supplement).
Analysis of weight difference between interventions
Orlistat vs LFRD
Comparison of the mean weight change in all the orlistat placebo groups (−3.7kg, 95%CI [-3.8, −3.5]) to the mean difference between the LFRD and the control groups (−4.8kg, 95%CI [-6.2, −3.4]) found a 1.1kg difference (95%CI [-0.3, 2.6] P=0.06).
Comparison of the mean weight change using the completer data for orlistat placebo groups (−2.2kg, 95%CI [-2.5, −1.9]) to the mean difference between the LFRD and the control groups (−4.8kg, 95%CI [−6.2, −3.4]) found a 2.6kg difference (95%CI [1.1, 4.0] p<0.001).
Comparison of the LOCF data for the orlistat placebo groups from trials which had provided completer data (−4.6kg, 95%CI [-4.8, −4.3]) to the mean difference between the LFRD and the control groups (−4.8kg, 95%CI [-6.2, −3.4]) found a 0.2kg difference (95%CI [-1.2, 1.7] p=0.38).
Liraglutide vs LFRD
Comparing the estimated mean weight change of the liraglutide placebo groups (−2.7kg) to the mean difference between the LFRD and the control groups (−4.8kg, 95%CI [-6.2, −3.4]) found a 2.1kg difference.
Semaglutide vs LFRD
Comparing the estimated mean weight change of the liraglutide placebo groups (−2.8kg) to the mean difference between the LFRD and the control groups (−4.8kg, 95%CI [-6.2, −3.4]) found a 2.0kg difference.
DISCUSSION
Comparison of weight change seen in all orlistat placebo groups to the difference between the LFRD and control groups found a 1.1kg non-significant difference with less weight loss in the placebo groups. Adjusting values to BOCF for participants that dropped out in trials that also provided data for completers resulted in a 2.6kg significant difference between the placebo and the difference between the LFRD and control groups, with less weight loss seen in the placebo groups. Using LOCF data from trials that also provided completer data found a 0.2kg difference between weight change in the placebo groups and the difference between the LFRD and control groups, with less weight loss in the placebo groups.
In liraglutide RCTs, comparison of weight change seen in the placebo groups to the difference between the LFRD and control groups found a 2.1kg difference. Placebo groups lost less weight than the diet groups.
For semaglutide RCTs, comparison of weight change seen in the placebo groups to the difference between the LFRD and control groups found a 2.0kg difference with less weight loss in placebo groups.
As far as we are aware, this is the first review to assess compensatory lifestyle changes following the induction of AOMs. Although differences in weight loss seen between AOM RCTs and LFRD RCTs may be due to compensation, dissimilarities in the trial design and populations studied may also have explained differences.
12/16 orlistat RCTs included run-in periods prior to randomisation in their design. Run-in periods identify non-compliers and rule them out of randomisation. This is thought to decrease the number of dropouts during the study, improve compliance and hence, reduce the bias from incomplete data while improving the apparent effectiveness of the drug33. They may, however, cause problems regarding weight loss results. Most weight loss occurs early, and a rapid weight loss during the run-in period may result in less weight loss seen during the active intervention34. Although this may affect weight change results in orlistat RCTs, run-in periods were not included in the design of 6/7 liraglutide RCTs and 5/5 semaglutide RCTs, meaning the limited weight loss seen in placebo groups of these trials cannot be due to early weight loss prior to randomisation.
PA advice was reported as being given to participants in 10/16 orlistat RCTs, 7/7 liraglutide RCTs and 5/5 semaglutide RCTs, however, LFRD RCTs providing PA advice were excluded to allow for comparability to orlistat RCTs often with no PA advice described. Diet with PA produces more weight loss than diet alone35; meaning participants in most of the AOM RCTs may be likely to experience more weight loss than those in the LFRD RCTs. However, reported advice given to participants of RCTs was often vague and undetailed, the advice given may not have significantly affected the amount of weight loss experienced.
Baseline BMI was higher in orlistat RCTs than LFRD RCTs, and even more so in liraglutide and semaglutide RCTs. Varying evidence has been found regarding baseline BMI and the degree of weight loss experienced36. Features such as higher waist circumference, total body weight, fat-free mass, and muscle mass have been correlated to weight loss success37, meaning those in AOM RCTs may be more likely to experience weight loss success.
AOM RCTs included a higher ratio of female participants than LFRD RCTs. A systematic review and meta-analysis of RCTs found no significant gender differences38. However, due to RCTs providing limited details regarding interventions, it was not clear whether dietary prescription took account of body size in men and women. Regardless, gender differences between included RCTs should not significantly affect results.
Previous weight loss attempts of participants were not reported in any RCT. Participants with previous attempts at weight loss are typically less successful subsequently, with speculation that this is due to treatment resistance39. Since lifestyle attempts at weight loss are typically tried prior to AOM initiation, participants in AOM RCTs may have an element of treatment resistance and thus see less weight loss than expected.
AOM RCTs were all sponsored by their drug manufacturing company, increasing the risk of bias for these trials. Trials funded by pharmaceutical companies are more likely to report results favouring the drug40. As previously mentioned, reported information regarding lifestyle advice given to participants was very limited. It could be speculated that drug companies limit advice given to participants, which might enhance the drug effect. This would also result in less weight loss than expected, particularly for those in the placebo groups.
There were significant numbers of dropouts in AOM RCTs. Both liraglutide and semaglutide RCTs encouraged participants to continue to attend visits regardless of whether they were still taking the drug, reducing the amount of missing data. On the other hand, orlistat RCTs did not report encouraging participants to return, resulting in missing data that were subsequently substituted with LOCF data by the drug company. This method, however, assumes weight remains the same following withdrawal28. Participants typically have a period of weight regain following the initial weight loss41. Where participants drop out before weight is regained, LOCF data provided participants with a better result than if they were to remain in the trial. Adjustment to BOCF data was conducted for these participants28. BOCF would mean that all participants dropping out would return to their baseline weight, which also may not be the case. Both scenarios are not ideal41.
The difference in weight change between the LFRD group and control of LFRD RCTs was compared to the pooled mean weight change of the placebo groups of AOM RCTs. Conversely, a pooled mean for weight change for the LFRD intervention groups alone could have been used as comparison. This was calculated to be −4.9kg (95%CI [-5.4, −4.3]), 0.1kg more than data used, yielding a slightly greater difference in weight change seen than between placebo groups and LFRD groups. Another systematic review comparing low-fat diets to other diets, including usual diet 42, found a weighted mean difference between low-fat diet and usual diet of −5.43kg (95%CI [-7.29, −3.54]). Using these data would result in greater differences in weight change seen between placebo groups and LFRD groups. Our data, therefore, allowed for a more conservative approach in analysis.
The follow-up period was limited to 12 months, or 68 weeks for semaglutide RCTs, to allow for a common follow-up time. This timeframe reflects long-term weight loss, with weight loss interventions commonly seeing rapid weight loss early followed by a period of weight regain34. LFRD RCTs were required to include no PA advice to allow comparison to orlistat RCTs that often did not include PA advice. Several orlistat RCTs did, however, include PA advice and removing this from the exclusion criteria for LFRD RCTs would allow for more studies to be included in this group of trials. We only examined AOMs which have a licence in the UK. These analyses could be extended to other medications. We also did not examine drug trials where meal replacements were used, which would then be compared to trials of weight loss including meal replacements.
Further research is necessary to assess compensatory behaviours following the initiation of AOMs. One way of assessing this might be to conduct a 3-armed crossover RCT of drug and LFRD versus placebo and LFRD versus LFRD, where all participants could eventually receive the study drug. This would allow for comparison between groups while ensuring advice received by participants was the same. Cohort studies assessing lifestyle changes in relation to AOM initiation would also be helpful. Assessing the impact findings have on the economic evaluation of AOMs, where differences between drug and placebo groups are used, is essential. Finally, it would be important to conduct interviews with patients and doctors about their experiences with AOMs and their beliefs on how initiation affects lifestyle behaviours.
CONCLUSION
Compensation for lifestyle measures may result following the initiation of AOMs. This could mean pharmacological management of obesity may not result in as much weight loss as expected with initiators gradually reverting to or continuing more of their unhealthy behaviours than expected. However, it may also be possible that participants of AOM RCTs have “treatment resistance” and hence, find it more difficult to lose weight through lifestyle behaviours. Regardless, for those starting anti-obesity medications, it is important to stress the importance of continuing caloric restriction and PA alongside the drug. Further studies are needed to assess these behaviours following the initiation of AOMs.
Data Availability
All data used are available from the following papers: Abbenhardt et al. 2013 https://doi.org/10.1111/joim.12062, Anderssen et al. 1995. Oslo Diet and Exercise Study: a one year randomized intervention trial. Effect on hemostatic variables and other coronary risk factors. Nutrition Metabolism and Cardiovascular Diseases vol 5. Astrup et al. 2012 https://doi.org/10.1038/ijo.2011.158, Bakris et al. 2002 https://doi.org/10.1097/00004872-200211000-00026, Berne 2005 https://doi.org/10.1111/j.1464-5491.2004.01474.x, Broom et al. 2002 http://www.ncbi.nlm.nih.gov/pubmed/12296610, Davidson et al. 1999 https://doi.org/10.1001/jama.281.3.235, Davies et al. 2021 https://doi.org/10.1016/S0140-6736(21)00213-0, Davies et al. 2015 https://doi.org/10.1001/jama.2015.9676 Finer et al. 2000 https://doi.org/10.1038/sj.ijo.0801128 Garvey et al. 2022 https://doi.org/10.1038/s41591-022-02026-4 Garvey et al. 2020 https://doi.org/10.2337/dc19-1745 Hauptman et al. 2000 https://doi.org/10.1001/archfami.9.2.160 Hollander et al. 1998 https://doi.org/10.2337/diacare.21.8.1288 Jones et al. 1999 https://doi.org/10.1016/S0895-7061(99)00123-5 Kadowaki et al. 2022 https://doi.org/10.1016/S2213-8587(22)00008-0 Kelley et al. 2002 https://doi.org/10.2337/diacare.25.6.1033 Krempf et al. 2003 https://doi.org/10.1038/sj.ijo.0802281 Lim et al. 2010 https://doi.org/10.1016/j.numecd.2009.05.003 Lindgarde 2000 https://doi.org/10.1046/j.1365-2796.2000.00720.x Miles et al. 2002 https://doi.org/10.2337/diacare.25.7.1123 O Neil et al. 2018 https://doi.org/10.1016/S0140-6736(18)31773-2 Pi-Sunyer et al. 2015 https://doi.org/10.1056/nejmoa1411892 Pritchard et al. 1999. https://doi.org/10.1136/jech.53.5.311 Rossner et al. 2000 https://doi.org/10.1038/oby.2000.8 Rubino et al. 2022 https://doi.org/10.1001/jama.2021.23619 Sjostrom et al. 1998 https://doi.org/10.1016/S0140-6736(97)11509-4 Swinburn et al. 2005 https://doi.org/10.1111/j.1463-1326.2004.00467.x Swinburn et al. 2001 https://doi.org/10.2337/diacare.24.4.619 Torgerson et al. 2004 https://doi.org/10.2337/diacare.27.1.155 Wadden et al. 2020 https://doi.org/10.1002/oby.22726 Wilding et al. 2021 https://doi.org/10.1056/nejmoa2032183 Wood et al. 1991 https://doi.org/10.1056/NEJM199108153250703 All data produced in the present work are contained in the manuscript
Conflict of interest
MM none declared. AA was funded as a research registrar for two of the included orlistat trials 1993-1995.
Funding
The Health Services Research Unit is funded by the Chief Scientist Office of the Scottish Health and Social Care Directorates.
Acknowledgements
We thank Paul Manson, Information Specialist at the Health Services Research Unit, University of Aberdeen, for assistance with search strategies.
ONLINE SUPPLEMENT

Modified PRISMA diagram for all included randomised controlled trials

Forest plot for meta-analysis of the effect of orlistat versus placebo on the number of dropouts at 12 months follow-up

Forest plot for meta-analysis of the effect of LFRD versus control on the number of dropouts at 12 months follow-up

Forest plot for meta-analysis of the effect of liraglutide versus placebo on the number of dropouts at 12 months follow-up

Forest plot for meta-analysis of the effect of semaglutide versus placebo on the number of dropouts at 68 weeks follow-up

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Last observation carried forward analysis of weight change in kg for orlistat trials
ABBREVIATIONS
- PA
- physical activity
- AOM
- anti-obesity medications
- GLP-1
- glucagon-like peptide-1
- LLD
- lipid lowering drugs
- RCT
- randomised controlled trial
- kcal
- kilocalorie
- BMI
- body mass index
- LFRD
- low-fat reducing diet
- kg
- kilogram
- SD
- standard deviation
- LOCF
- last observation carried forward
- RR
- risk ratio
- CI
- confidence interval
- BOCF
- baseline observation carried forward
REFERENCES




