
Abstract
Thrombophilia is defined as the willingness of blood to clot easily in a situation of imbalances between fibrinolysis and coagulation. It is classified as inherited and acquired thrombophilia. Several studies revealed that the inherited thrombophilia is strongly associated with single nucleotide polymorphisms (SNP) or deletions on certain genes, such as FV Leiden (rs6025), MTHFR1 (rs1801133), MTHFR2 (rs1801131), Serpine-1 (rs1799768), and Factor II (rs1799963). This study aims to develop an SNP detection panel based on Kompetitive Allele Specific Primer-polymerase chain reaction (KASP-PCR) technique. Results revealed that 86.5% of susceptible patients (n = 111) contain at least one mutation; while seven of them harbor three thrombophilia-associated mutations simultaneously. A clear allelic discrimination was observed for all tested samples. The prevalence of each mutation among different countries and ethnic groups are in line with the findings of this study. Rather than expensive and time-consuming approaches, the current assay enables the cost-effective advantage of the KASP-PCR, which reduces the diagnostic cost with a fast and convenient way. After clinical validation and approval, it can be used in hospitals, research centers, and diagnostic laboratories to determine the genetic susceptibility of individuals to thrombosis and for research purposes.
Introduction
Thrombophilia is defined by the World Health Organization/International Society of Thrombosis and Hemostasis (WHO/ISTH) as an abnormal tendency to coagulation or clotting of the blood in a part of the circulatory system (WHO, 1995). The disease poses a significant health burden. According to the CDC reports, >900,000 people in the United States alone are affected by blood clots each year, with substantial mortality rates. Due to thrombophilia-related complications, 60,000 to 100,000 deaths are recorded in the USA annually, which is greater than the total number of people who lose their lives each year from AIDS, breast cancer, and motor vehicle crashes combined (Badireddy & Mudipalli, 2022). The disease is classified as inherited and acquired thrombophilia. Inherited thrombophilia is associated with four SNPs and one deletion mutations located in different genes, namely: coagulation factor II (FII), coagulation factor V (FV), 5,10-methylene tetrahydrofolate reductase (MTHFR1 and MTHFR2), and serpine1 (SERPINE1) (Yapijakis et al, 2015).
Diagnostic approaches include detecting disorders by examining clinical signs, imaging techniques, and analysis through molecular aspects. Direct DNA genotyping, PCR-based techniques, immunological detection, and chromogenic assays are used to identify thrombophilia-related disorders (Linnemann and Hart 2019). Sequencing techniques are the most accurate approaches followed and used for validation purposes. On the other hand, PCR-based approaches such as TaqMan, KASP and rhAmp are mostly used due to their simplicity, timesaving, cost-effectiveness, and ability to measure the heterozygosity or homozygosity of mutations carried among thrombophilia genes.
Kompetitive Specific Allele Primer-PCR (KASP-PCR) is a fluorescent-based reporting system to identify and measure the SNPs (He et al., 2014). It is used to differentiate between species in plants and animals (Yang et al., 2020). KASP-PCR technique is fast, sensitive, relevant, and cost-effective (Alvarez-Fernandez et al., 2021; Zhang et al., 2020). Due to the cost advantage, it has been applied widely in plant breeding for commercial use (Makhoul et al., 2020). KASP technique is precise, and its specificity is based on the competitive nature of allele specific forward primers and modified Taq polymerase.
The current genotyping techniques are based on sequencing or PCR, which are time consuming and expensive methods. Therefore, a cost-effective, time-saving, and accurate technique is needed to screen symptomatic and asymptomatic suspicious people. This study aims to screen thrombophilia associated SNPs based on KASP-PCR technique. For this purpose, the DNA samples of thrombophilia-susceptible patients (n = 111) were collected and five associated mutations on FV Leiden, MTHFR1, MTHFR2, Serpine-1, and Factor II genes were identified. Rather than expensive and time-consuming approaches, the current assay reduces the diagnostic cost in a fast and convenient way.
Material and Methods
Collection of blood samples and ethical concerns
5 mL of leftover whole blood samples were retrieved from King Fahad Military Medical Complex (KFMHC) (IRB Protocol No: AFHER-IRB-2022-031). A total of 111 samples have been collected from thrombophilia-susceptible patients who have been admitted to the hospital with thrombophilia symptoms, such as chest pain, abdominal pain, dizziness, fever, seizure, breath shortness, etc. The blood samples were collected in an Ethylenediamine tetra acetic acid tube (EDTA) and stored at −20 °C until DNA extraction.
Extraction of DNA
QIAamp® DNA Blood Mini Kit 250 (QIAGEN) was used to extract and purify DNA. The instructions of the manufacturer were followed. The final eluate was kept at −20 °C for further stages. NanoDropTM 2000/2000c spectrophotometer was used to quantify the purity and concentration of extracted DNA samples. The samples were also visualized in agarose gel for 20 min at 100 Volt and monitored under UV light (Molecular Imager® ChemiDoc™ XRS+, Bio-Rad). Image Lab™ Software (Bio-Rad) was utilized to save the images.
Primer design
Primers corresponding to the SNP positions were manually designed. First, the corresponding gene sequences were retrieved from NCBI database (https://www.ncbi.nlm.nih.gov) and Primer Blast tool was used to pick the primers. In addition, Primer 3 program was used to verify the designed primers: one common reverse, two alternating forward primers that are specific to the SNP positions.
Validation of plate reader and KASP-PCR reaction
Before genotyping, KASP genotyping validation kit (LOW ROX KASP TF Validation kit, LGC) was used to validate the plate-reader instrument (7500 Fast Real-Time PCR System). According to the manufacturer’s protocol, the compatibility and readability of the plate reader was confirmed. The kit consists of three tubes of diluted fluorophores: FAM, HEX, and HEX/FAM. The tubes were briefly vortexed and dispensed into a microtiter plate. Then, KASP reagents (2x KASP master mix, and 72x KASP assay mix) with provided DNA samples (n = 36) were used to run the following protocol: (1) 94 °C 15 minutes for activation (1 cycle); (2) 94 °C 20 sec for denaturation and 61-55 °C 60 sec (drop 0.6 °C per cycle) for annealing/elongation (10 cycles); (3) 94 °C 20 sec for denaturation and 55 °C 60 sec for annealing/elongation (26 cycles). At the end of the reaction, the endpoint fluorescent reading was performed. To obtain the best genotyping clusters, the plate underwent two rounds of recycle steps, as follows: 94 °C 20 sec for denaturation, and 57 °C for 60 sec for annealing/elongation (3 cycles).
Genotyping of thrombophilia-associated SNPs with KASP-PCR
The KASP primer mixture for each target SNPs was prepared including 12 µl of forward-1 primer, 12 µl of forward-2 primer, 30 µl of common reverse primer, and 46 µl of distilled water to reach the total volume of 100 µl. Then, 5 µl of master mixture (KASP™ TF Low ROX Master Mix) and 0.14 µl of assay mixture were added and vortexed briefly. In 96 well plate, 5 µl of assay mixture was added with 5 µl of DNA sample in each well and then sealed tightly. The KASP genotyping assay was performed by using real-time PCR 7500 (Applied Biosystem) instrument.
RESULTS
Calibration and optimization of KASP protocol
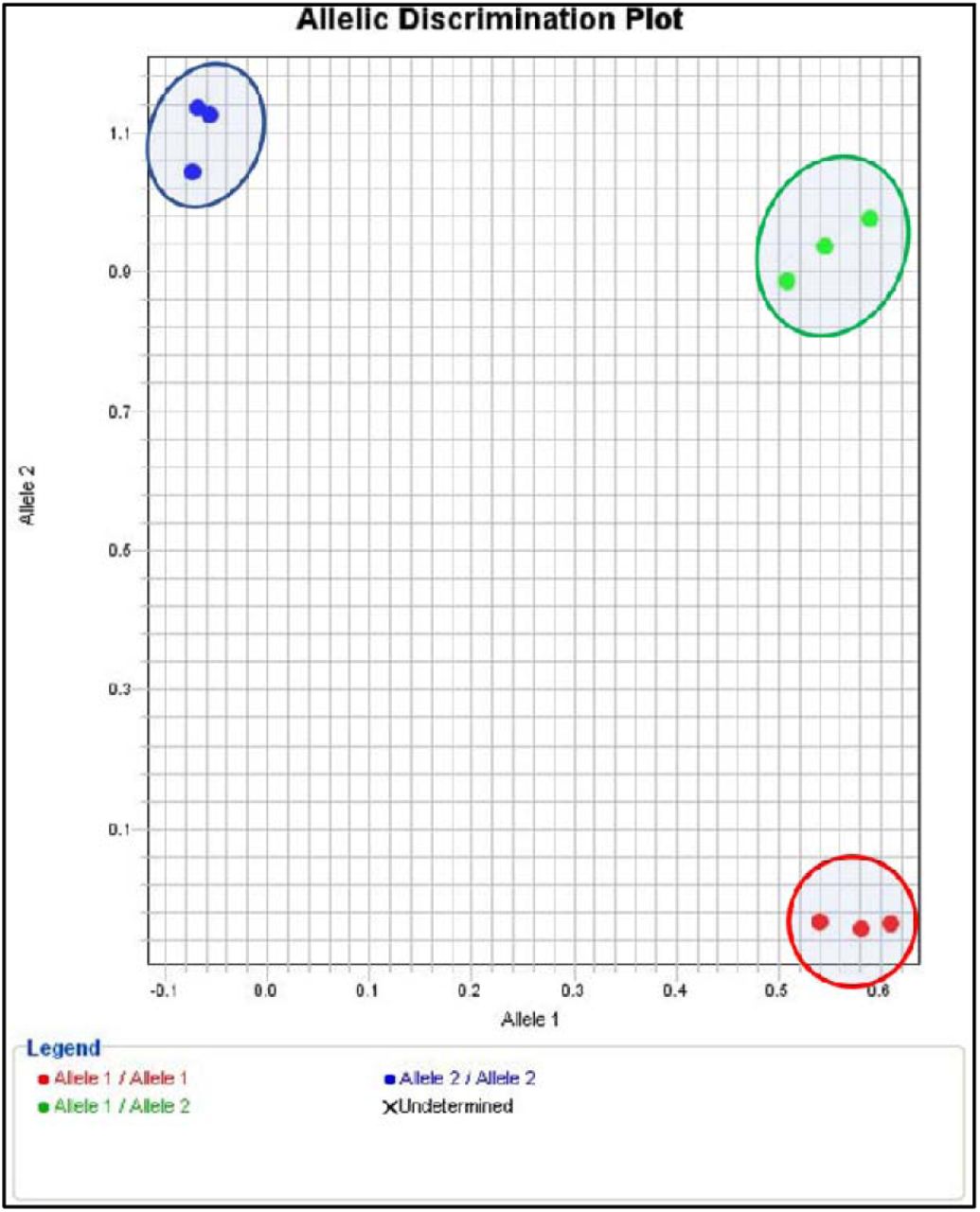
Before the KASP-PCR reaction for the discrimination of thrombophilia-associated SNPs, the validity of the fluorescent thermal cycler and the protocol for KASP-PCR were optimized and validated. Nine positive control samples (LGC Bioscience), labeled with FAM (blue), HEX (red), and FAM/HEX (green) fluorophores, were used to optimize, and verify the fluorescence signals that will be obtained from the thermal cycler. Figure 1 depicts the cluster plot of FAM, HEX, and FAM/HEX labeled positive control samples. The clusters correspond to homozygote dominant (allele 1/allele 1), homozygote recessive (allele 2/allele 2), and heterozygote (allele 1/allele 2) discriminations. This result showed optimized and successful KASP-PCR reaction conditions with calibrated fluorometric measurements.
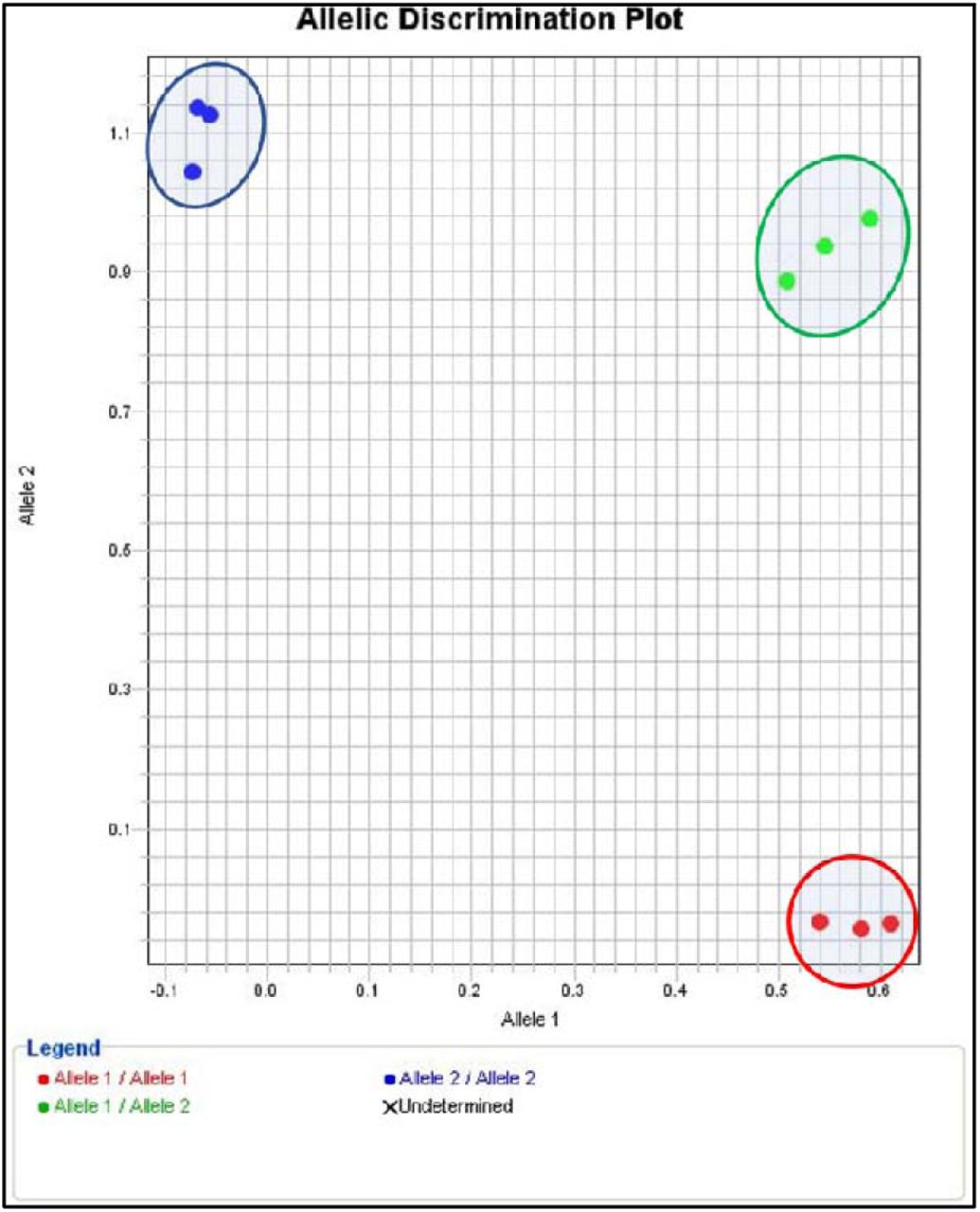
The allelic discrimination plot of FAM (blue), HEX (red) and FAM/HEX (green) fluorophores. Three samples used for each positive control dyes.
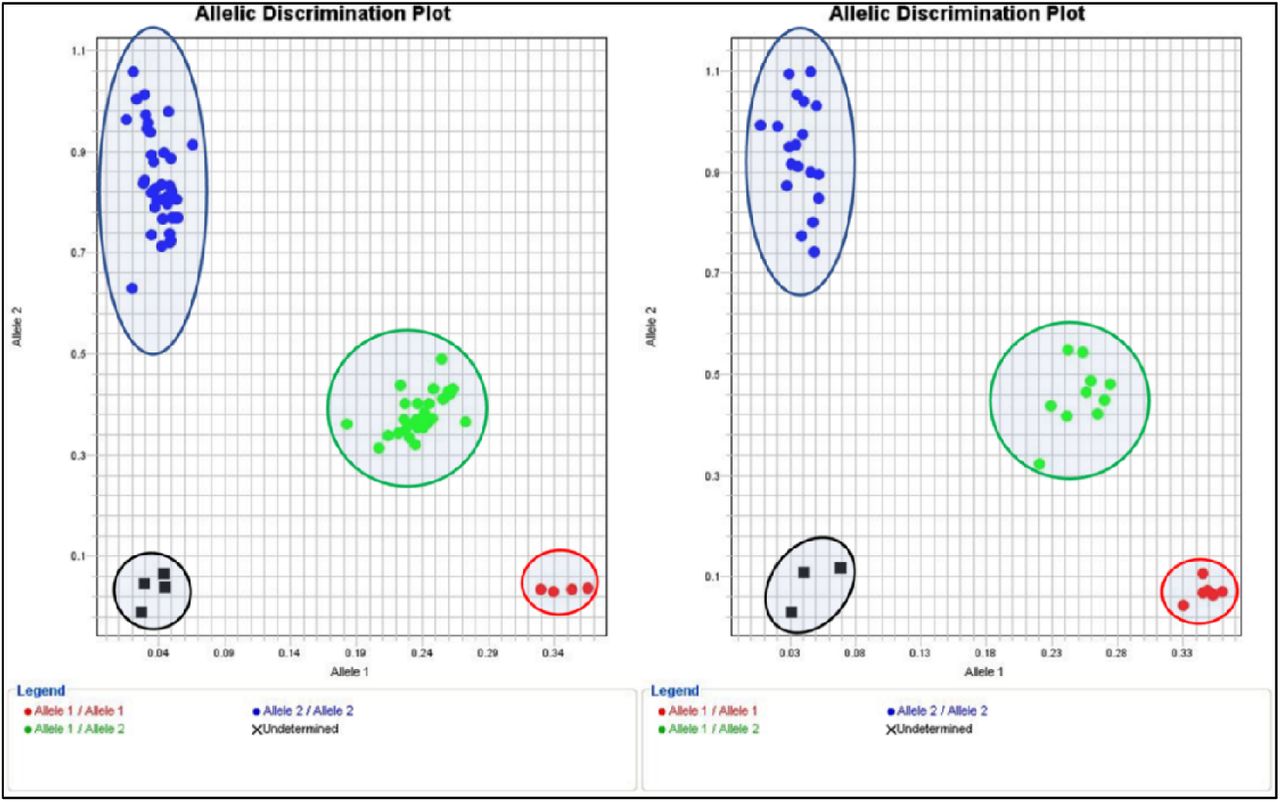
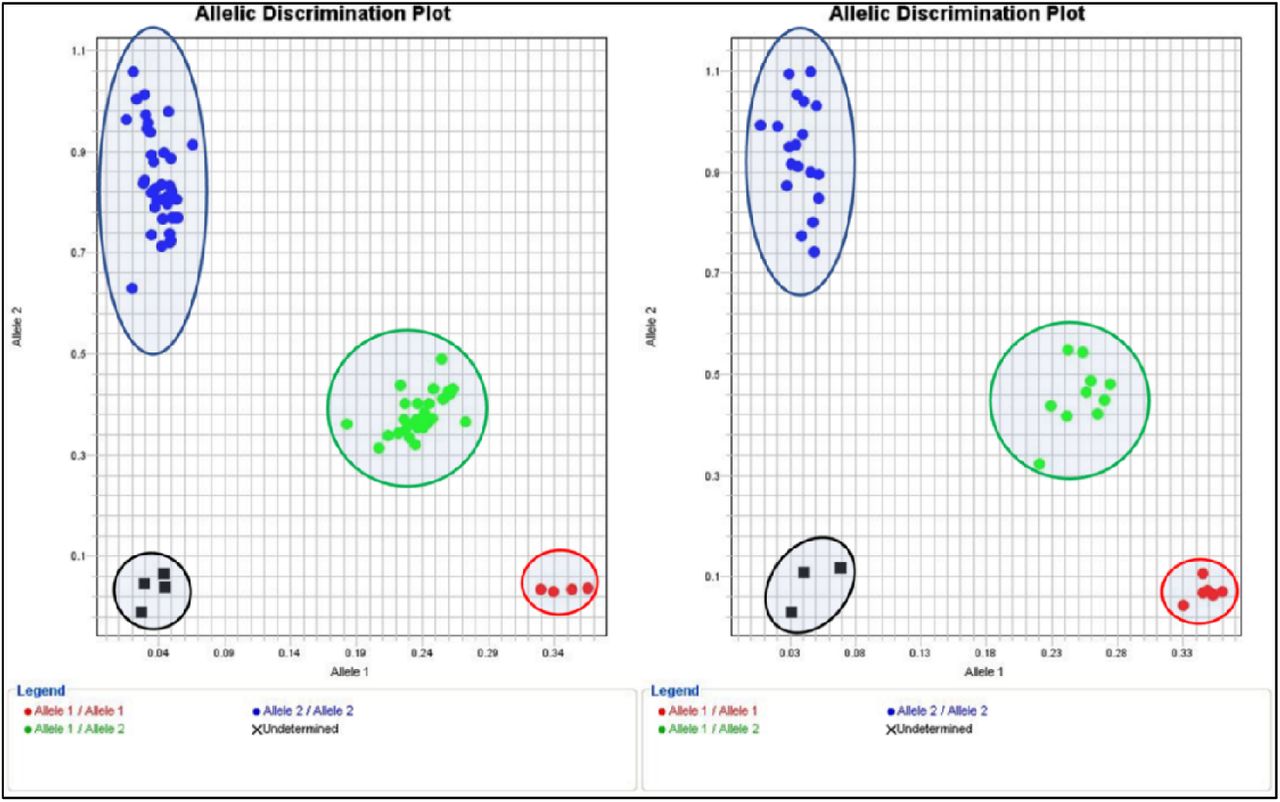
Furthermore, the optimized protocol was used to discriminate real DNA samples (n = 45) provided by the LOW ROX KASP TF Validation kit (LGC Biosciences). In addition to the DNA samples, three negative control samples were included. After the KASP-PCR reaction, the allelic discrimination plot was depicted in Figure 2. The results were shown before (Figure2A) and after three (Figure2B) and six (Figure2C) additional recycling stages. After six recycling stages, positive and negative samples were clearly separated, and the negative control specimens were placed near the origin side of the plot. In addition, the homozygote and heterozygote alleles were determined to be well-clustered. It is obvious that additional recycling steps improved the allelic discrimination, where the best and most efficient results were obtained upon six additional recycling stages (Figure 2C).

Validation of plate reader and KASP-PCR protocol. Allelic discrimination plot of DNA samples (n = 45). A) Without recycle step. B) After the addition of three recycling steps. C) After the addition of six recycling steps. Black dots indicate the negative control sample. Red, blue, and green dots indicate the homozygotes of Allele 1, homozygotes of Allele 2, and heterozygotes of Allele 1/2.
KASP-PCR genotyping of rs6025 (G1691A) on the Factor V Leiden gene
An optimized KASP-PCR protocol was performed to identify the G1691A substitution on the FVL mutation (FV gene, rs6025). Figure 3. shows the discrimination plots of samples. Since the total sample number (n = 111) is more than the capacity of the thermal cycler (n = 96), the reaction was completed in two separate runs. Upon the KASP-PCR reaction, an additional six recycling steps was added for the best reaction performance. Black dots indicate negative control, green dots indicate heterozygote sample (CT), and blue dots indicate homozygote (CC). Accordingly, only one sample was detected as heterozygote (∼1%), and the rest of the samples were homozygote wild (∼99%). This result shows that almost all thrombophilia-susceptible individuals admitted to the hospital are free of FVL gene mutation.

The figure shows the discrimination plot of FVL mutation with an additional 6 cycles. Black dots indicate negative control, green dot indicate heterozygote sample (CT), and blue dots indicate homozygote wild (CC).
KASP-PCR genotyping of (rs1799963) (G20210A) on the FII gene
KASP-PCR assay was performed to screen the G20210A variation on the FII-PT gene. Figure 4.1 depicts the discrimination plots of extracted DNA samples. Since the capacity of the PCR plate is 96 wells, the run was divided into two runs. In addition to the KASP-PCR thermal cycle, six more recycling step was added to improve discrimination. Black dots refer to negative control, placed near the plot’s origin side; blue dots refer to homozygote wild samples (GG); red dot sample is homozygote mutant (AA), while no green dots of heterozygote recorded. Only one sample was recorded as homozygote recessive, while the rest of the sample was homozygote dominant, and no heterozygote detected. This result shows that only one of the susceptible thrombophilia patients carried the FII-PT mutation.

Shows the discrimination plot of Factor II mutation with an additional 6 cycles. Black dots indicate negative control, blue dots indicate homozygote wild (GG), and red dots indicate homozygote mutant (AA).
KASP-PCR genotyping of (rs1801133) on the MTHFR gene
After optimization of the KASP-PCR assay, screening for mutation on MTHFR1 was performed (MTHFR gene, rs1801133). Figure 25 illustrates the discrimination plot of susceptible-thrombophilia patient samples. The reaction was completed in two runs due to the number of samples (n=111). In addition, six recycling steps were added to obtain clear discrimination. Four black dots refer to negative control and are correctly placed near the origin of the plot, green dots refer to the heterozygote sample (CT), and red dots refer to the homozygote sample (CC). Consequently, 24 % of the patients were heterozygote, only two samples were recorded as homozygote recessive (TT) (∼2%), and the rest of the samples were recorded as homozygote dominant. This result shows that ∼26% of the patients admitted to the hospital with a risk of developing thrombophilia are carrying at least one allele of MTHFR1 mutation.
KASP-PCR genotyping of (rs1801131) on the MTHFR2 gene
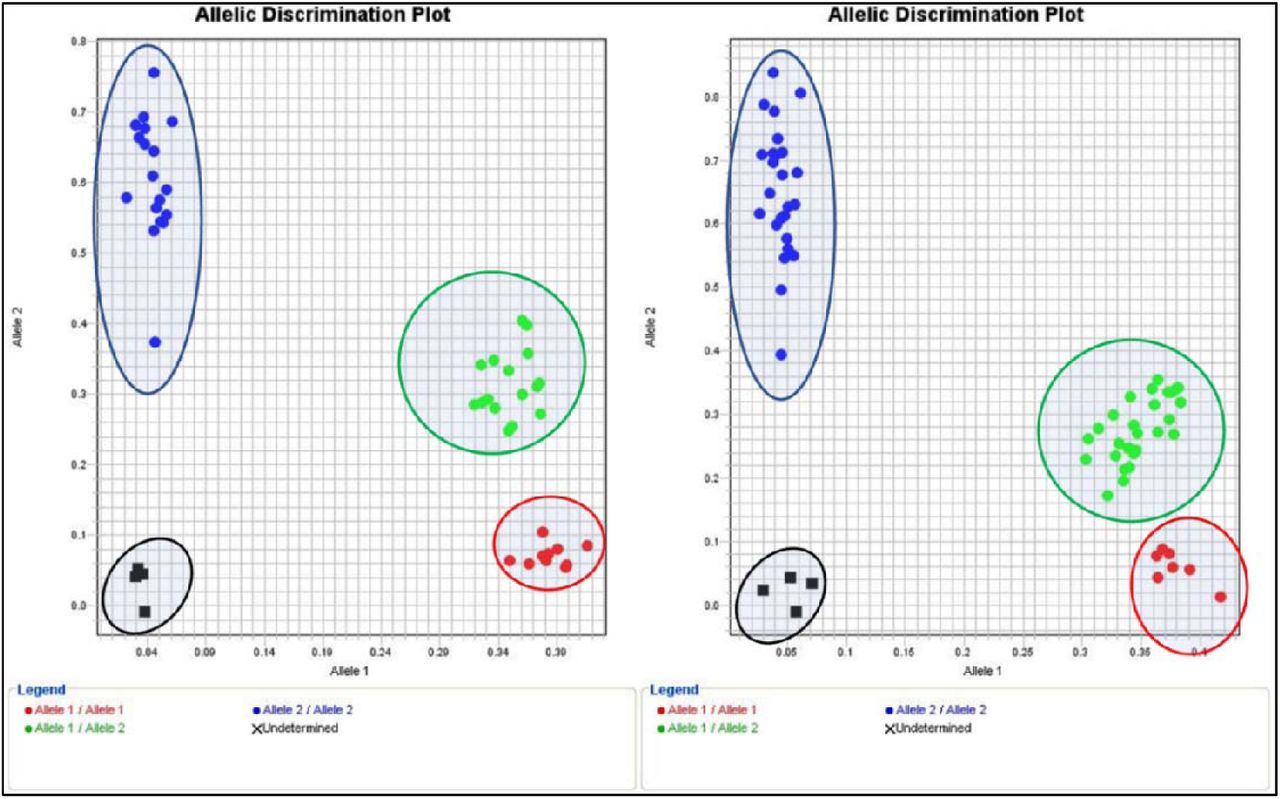
An optimized KASP-PCR assay was achieved to screen the mutation placed on the MTHFR2 gene (rs1801131). Figure 3 demonstrates the discrimination plot of two runs performed on extracted DNA samples. With the addition of six thermal recycling steps, the reaction shows the best performance. Black dots imply negative control; green dots imply heterozygote sample (AC), blue dots imply homozygote wild (AA), and red dots imply homozygote recessive (CC) alleles. Discrimination results showed that ∼53% of the patients admitted to the hospital are free of mutation (wild), 39% carrying this mutation in one allele, and 6.3% carrying two alleles of mutation. The result shows that ∼45% of susceptible thrombophilia patients have at least one mutation.

Shows the Allelic Discrimination Plot of MTHFR rs1801133 (C/T) mutation with an additional 6 cycles. Black dots indicate negative control; green dots indicate heterozygote (CT); and red dots indicate homozygote mutant (TT); blue dots indicate homozygote.
Shows the Allelic Discrimination Plot of MTHFR rs1801131 mutation with the addition of 3 cycles. Black dots indicate negative control; red dots indicate homozygote mutant (CC), green dots indicate heterozygote (AC), and blue dots indicate homozygote wild.
KASP-PCR genotyping of Serpine 1 (rs1799768)
Genetic screening for Serpine 1 (rs1799768) mutation was performed by optimized KASP-PCR assay. Figure 7 shows the discrimination plot of the (n=111) sample divided into two runs due to the capacity of the thermal cycler. Black dots indicate negative control, and it is successfully placed near the origin of the plot; blue dots indicate homozygote dominant 5G/5G, green dots indicate heterozygote 5G/4G and red dots indicate homozygote recessive 4G/4G. Unlike other genes, only three additional thermals are needed to obtain clear discrimination of samples. Therefore, 47 of the sample was detected as homozygote dominant (∼42%), 44 of the sample were detected as heterozygote by carrying one mutation (∼39%), and 17 were detected as homozygote recessive (∼15%). The result shows that more than 50% of patients harbor Serpine 1 mutation, which increases the risk of developing thrombophilia.

Shows the discrimination plot of Serpine 1 rs1799768 mutation with an additional 3 cycles. Black dots indicate negative control, red dots indicate homozygote mutant (4G/4G), green dots indicate heterozygote (5G/4G), and blue dots indicate homozygote wild.
DISCUSSION
This study aims to screen genetic risk factors in patients susceptible to thrombophilia disease by applying the cost-effective PCR technique (KASP-PCR). For this purpose, left-over blood samples (n = 111) collected from thrombophilia symptomatic patients were utilized for genetic screening. Approximately 30% of the cases were admitted to the hospital with chest pain and 20% with abdominal pain. In addition to these symptoms, vomiting (2.7%), shortness of breath (11%), palpitations (4.5%), dizziness (10%), and fever (5.5%) were among the most common symptoms recorded. Patients who apply to the hospital with suspicion of the disease are aged 5-92 (mean = 52), male and female (62 male, 50 female).
KASP-PCR analyses revealed that 92 out of 111 (∼83%) patients susceptible to thrombophilia carry at least one of the analyzed mutations. The age and gender were not found to be associated with thrombophilia-related polymorphisms (P >0.05). Before KASP-PCR genotyping testing, the KASP genotyping validation kit was used to optimize and validate the plate reader. The device was calibrated according to the passive reference dye ROX™ contained in the KASP master mixture. Optimal FAM, HEX, and FAM/HEX fluorescence signals were checked and adjusted for the most efficient signal score. Figure 1. shows successful discrimination in testing FAM, HEX, and FAM/HEX dyes; where FAM is clustered in the Y-axis direction, HEX is clustered in the X-axis opposite direction, while the FAM/HEX mixture is clustered in the middle. Moreover, the cycle and re-cycling stages were optimized to obtain the best allelic discrimination (Figure 2). Results revealed that two rounds of three re-cycling steps (six in total) provided the most efficient protocol for robust allelic discrimination.
The primary role of the FV gene is regulating the production of coagulation factor V protein. A mutation found in this gene (G1691A) substitutes arginine to glutamine amino acid at point 506 in a polypeptide of Factor V (Arg506Gln) (Madkhaly et al., 2021), leading to unresponsiveness to anticoagulant factors (C and S) (Kujovich, 2018). The risk of developing thrombophilia is five times higher in heterozygotes and 50 times higher in homozygotes, and it is responsible for 20-25% of all VTE cases (Bezgin et al., 2018). It was found to be the most critical genetic risk factor related to thrombophilia (Djordjevic et al., 2012). The prevalence of FVL among the European population is high, while it is rare in Eastern Asia and Africa. Since the Arab countries are geographically at the center. The prevalence of FVL mutation in different countries and ethnic groups are listed in Table 1. Our results showed that all collected samples are homozygote wild, except one sample which is heterozygote (No. 61). In Figure 3., the heterozygote individual was admitted to the hospital with flank pain and dysuria. A prospective study aims to evaluate the prevalence of FVL in 149 healthy Saudi subjects revealed that 2% of the individuals are heterozygotes, and none of those individuals are homozygotes mutant (0%) (Almawi et al., 2005). Golestani et al., (2022) investigated the correlation between acute myocardial infarction (AMI) and FVL in the Iranian population; 5.5% of cases were found to be heterozygotes, while 1% were homozygote mutants. On the other hand, Gowda et al., (2000) found that among American subjects, 8% were heterozygote. Based on these results, the data in the literature is in line with and compatible with our results.
Prothrombin is a protein synthesized in the liver and is essential in clotting the blood (Khan & Dickerman, 2006). As a result of the replacement of guanine with adenine at position 20210 of the coagulation factor II (FII) gene (G20210A), high concentrations of prothrombin protein are activated (Poudel et al., 2020; Ahmed et al., 2020; Rennert & DeSimone, 2019). An increase in prothrombin level increases thrombin level and inhibits Activated Protein C (APC) - inhibits FV protein-, subsequently stimulating thrombus formation. Thus, the risk of VTE appearance increases. It is estimated to be the second most important genetic risk factor causing thrombophilia (Djordjevic et al., 2012). In our experiment, one out of 90 patients carry a homozygous mutant allele (Patient No. 52, 86 years old male, and suffering from dysuria); no mutation was detected in other samples (Figure 4.14). A study has been conducted to screen FII and FVL mutations from eight years-old patient who is suffering from dysuria and priapism. The genotyping result revealed that the patient was heterozygote for both mutations (Özbek et al., 2003). At the same time, the patient is homozygote with FII and heterozygote with FVL. A retrospective study showed that 2.6% of patients screened for FII are positive through Saudi thrombosis patients (Madkhaly et al., 2021). A cross sectional study investigate the prevalence of FII mutation in Jordanian population; 5.7% were heterozygote while 2% were homozygote mutant (Al-Zoubi et al., 2021). A group of healthy Arab population enrolled in a retrospective study to test the distribution of FII. No mutated allele among Saudis was observed, while 1% of heterozygotes in Bahraini. In Lebanese and Tunisian, 3.6% and 2.6% are heterozygotes, respectively (Almawi et al., 2005). An amplification refractory mutation detection system (ARMS) was applied to define the prevalence of FII in Chechans populations in Jordan; only 2% of heterozygotes were detected, while no homozygote mutant (Dajani et al., 2012). The fact that the mutation prevalence in the general population is 2-3% in the western region, while rare in other geographical regions and all previous literature shows a rare incidence of FII mutation, which reflects KASP-PCR results.
The MTHFR gene decreases homocysteine concentration by producing the MTHFR enzyme to convert the homocysteine to methionine (Hickey et al., 2013; Dean, 2016). Two recognized mutations in the MTHFR gene inactivate the enzyme, leading to increased levels of homocysteine and decreased levels of folate in plasma: C677T (rs1801133) and A1286C (rs1801131) (Dölek et al., 2007). The American Congress of Obstetricians and Gynecologists recommends screening for MTHFR mutations instead of homocysteine concentration in patients at risk of thrombophilia (Hickey et al., 2013). In our experiment, we detected these mutations using KASP-PCR method. The prevalence of C677T (rs1801133) was ∼2% with homozygote mutant, ∼24% heterozygote, and ∼75% homozygote wild (Figure 25). Whereas the prevalence of A1286C (rs1801131) was ∼6% homozygote, ∼40% heterozygote, and ∼55% homozygote wild (Figure 36). The prevalence of C677T among Hispanics is over 25% and between 10-15% among Caucasians and North Americans with homozygote type (Hickey et al., 2013). Dajani et al, (2013). Investigating the prevalence of C677T among Chechen and Circassians healthy individuals; 27.5% of Chechen carry the mutation, while 50% of Circassians. A study reported that 31% of patients with stroke carried heterozygosity of C677T, while 15% were homozygote mutants. The higher incidence of that variant is attributed to other risk factors, such as smoking and hypertension (Djordjevic et al., 2012).
A variation in the serpine 1 gene is represented by the deletion of 4G/5G alleles in position 675 in chromosome 7 at the promoter region (Xu et al., 2016; Isordia-Salas et al., 2009; Tsai et al., 2008). The role of the serpine1 gene is to synthesize plasminogen activator inhibitor 1 (PAI-1), and the mutation increases production (Morange et al., 2007). High concentration of PAI-1 leads to inhibit plasmin from fibrinolysis, causing to accumulate clots in veins (Heit MD, 2013; Morange et al., 2007; Kazuo Miyashita et al., 2012). The allelic discrimination of KASP-PCR of this mutation showed that ∼40% of samples are heterozygote, while 14.4% were detected as homozygote mutant (Figure 7. 7). In total, 54% of patients carried PAI-1 variation. Yapikajis et al., (2012) conducted a genotyping study using blood samples from a healthy Greek population, and 49% were found mutated. A case-control study was performed to define the correlation between high concentration of PAI-1 and developing ischemic stroke in young Indian patients. Akhter et al., (2017) found that 62% of young Indian patients have PAI-1 SNP. Xu et al., (2016) found that ∼46% of chronic obstructive pulmonary disease through Chinese Han patients were heterozygote, while ∼14% were homozygote mutants. These results are in line with the current findings (Table 1).
Conclusion
A gene panel covering five thrombophilia associated mutations (Serpine 1, MTHFR1, MTHFR2, Factor V Leiden, and Factor II) was developed based on the KASP-PCR assay to diagnose thrombophilia genetic risk factors. The variety of diagnostic tests, the unreliability of clinical judgment, and a delayed diagnosis could lead to illnesses that may increase mortality and morbidity. In addition, molecular-based analyses are highly costly and time-consuming to obtain accurate results compared to the KASP-PCR assay. The KASP-PCR assay is a cost-effective (∼2-3 dollar per reaction), timesaving (3-4 hours), non-invasive, accurate, and highly sensitive. In this study, we obtained a clear allelic discrimination for all samples tested to screen SNPs related to thrombophilia. Rather than expensive and time-consuming approaches, the current assay enables the cost-effective advantage of the KASP-PCR assay, which reduces the diagnostic cost with a fast and convenient way. After clinical validation and approval, it can be used in hospitals, research centers, and diagnostic laboratories to determine the genetic susceptibility of individuals to thrombosis and also for research purposes.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Authors’ contributions
HT and RA conceptualized the study. RA and HT conducted the experiments. RA, and HT wrote the manuscript. AA, TA, MA, HA, NA, AIA identified the patients and provided the samples. TU revised and commented on the manuscript.
Acknowledgment
This study is funded by the Deanship of Graduate Studies under project number 2023-003-IRMC. The figures are created with BioRender.com.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}