
ABSTRACT
The International Society for Clinical Densitometry convenes a Position Development Conference (PDC) every 2 to 3 years to make recommendations for guidelines and standards in the field of musculoskeletal measurement and assessment. The recommendations pertain to clinically relevant issues regarding the acquisition, quality control, interpretation, and reporting of measures of various aspects of musculoskeletal health. These PDCs have been meeting since 2002 and have generated 214 Adult, 26 FRAX, 41 pediatric, and 9 general nomenclature consideration positions, for a total of 290 positions. All positions are justified by detailed documents that present the background and rationale for each position. However, the linkage to these publications is not maintained by the ISCD or any other publication such that physicians cannot easily understand the etiology of the positions. Further, the wording of many positions has changed over the years after being reviewed by subsequent PDCs. This Scoping review captures the references, changes, and timeline associated with each position through the 2019 PDC. It is meant to serve as a guide to clinicians and researchers for intelligent use and application of the positions.
INTRODUCTION
The International Society for Clinical Densitometry (ISCD) is a non-profit professional organization dedicated to the advancement of assessment of musculoskeletal health, particularly (but not limited to) bone densitometry. A major focus of the ISCD is the development of guidelines and establishment of standards for bone densitometry, assessment of fracture risk, and other aspects of musculoskeletal measurement. The Society conducts Position Development Conferences (PCD) approximately every two to three years to develop guidelines and standards (expressed as Position Statements) for new technologies used to assess musculoskeletal health and fracture risk, and to update older guidelines and standards as new data become available. The ISCD Official Positions are widely used by clinicians and densitometry technologists as a reference regarding the indications for, acquisition of, and interpretation and reporting of measures of musculoskeletal health, as well as the incorporation of those measures into fracture risk assessment. The curricula of the densitometry educational courses provided by ISCD are largely based on these Positions.
The ISCD PDC process is designed to summarize and use the best scientific evidence available to develop and update Position Statements regarding musculoskeletal assessment. Since musculoskeletal assessment technologies are evolving, some clinically important issues are addressed in the absence of robust evidence and are largely based on expert opinion. However, the PDC process grades and highlights the limitations of the available evidence pertinent to each statement and indicates where additional research is needed to improve the scientific evidence on which Positions are based and to resolve areas of ambiguity and controversy.
The primary way for clinicians to learn about the positions and refer to them is through the official PDC documents from the ISCD for Adults, FRAX, and Pediatrics. The linkages back to the primary peer-reviewed publications, that serve as the rationale for each position, are not presented in these summary documents. Thus, it is very difficult to find the details on the positions, to know if the position is still valid, or is valid for a particular patient population. In this scoping review, each current position is linked to the ISCD summaries of its associated PDC where it was developed and to the associated publications. We also track the changes in wording, if any, that occurred in subsequent PDC.
Scoping Question
How and why have the ISCD positions evolved over time regarding the diagnosis of osteoporosis and the use of the densitometry system?
Rationale
Positions are broadly used in clinical practice and presented without reference to the core publications. Further, there are no means for practicing physicians and researchers to easily understand how the wording of a position has changed over time, the quality of the evidence, the regional applicability, and outstanding controversies associated with the creation of the position.
Objectives
The objective of the review is to capture each position statement and offer its etiology and pedigree.
METHODOLOGY
A Scoping review was performed following the methodological guidelines of Peters et al.2 A Scoping review was chosen versus a systematic review since all of the literature on the topic was from definitive resources but the clarity of the concepts and definitions of the positions had been lost over time. The protocol for this review is self-contained in this manuscript.
Eligibility criteria
We considered only the peer-reviewed accepted publications in the English language from the years 2001 through 2022 that were directly attributed to the deliberations of the task forces and executive committees of the PDCs.
Information sources
It was known a priori that all position papers were published in the Journal for Clinical Densitometry. PubMed, Google Scholar Search and Publish or Perish 3 were used to find all relevant documents and their associated citations. In addition to peer review publications, we used the most recent form of the Positions distributed by the ISCD. These consist of three documents found on their website 4: The 2019 ISCD Official Positions Pediatric, the 2019 ISCD Official Positions Adult, and the 2019 Official Positions in FRAX. The most recent search was performed in January, 2023.
Search
We used the following search parameters: Journal name: “Journal of Clinical Densitometry”; Keywords: “Position Development Conference”, “Positions”, “Executive Summary”; Years: 2003-2004, 2005-2006, 2007-2008, etc.
Selection of sources of evidence
Publications were selected that were a direct result of the PDC it was associated with and published by the participants. The relevant publications were generally in the form of an Executive summary that summarized new and previous positions were followed in the same issue by publications authored by each task force providing background and discussion on each question examined.
Data charting process
We took the approach of starting with the current ISCD position documents and their wording. We then traced back through all the identified Executive Summaries to find when each position was developed. We then noted exact wording changes since the conception of the position and reviewed the publications to determine the rationale for any wording changes. We organized the positions using the same headings and order one finds in the ISCD position documents. We gave each position a number prefixed by a letter signifying which document it is found with A=Adult, F=FRAX, P=Pediactric. We created a table that catalogs each position by the conference it was discussed and developed and the associated publications. Wording changes to each position are noted in the footnotes.
Synthesis of results
Besides tracking the wording changes for each position, we also note the relative citations related to the positions as a whole by years.
RESULTS
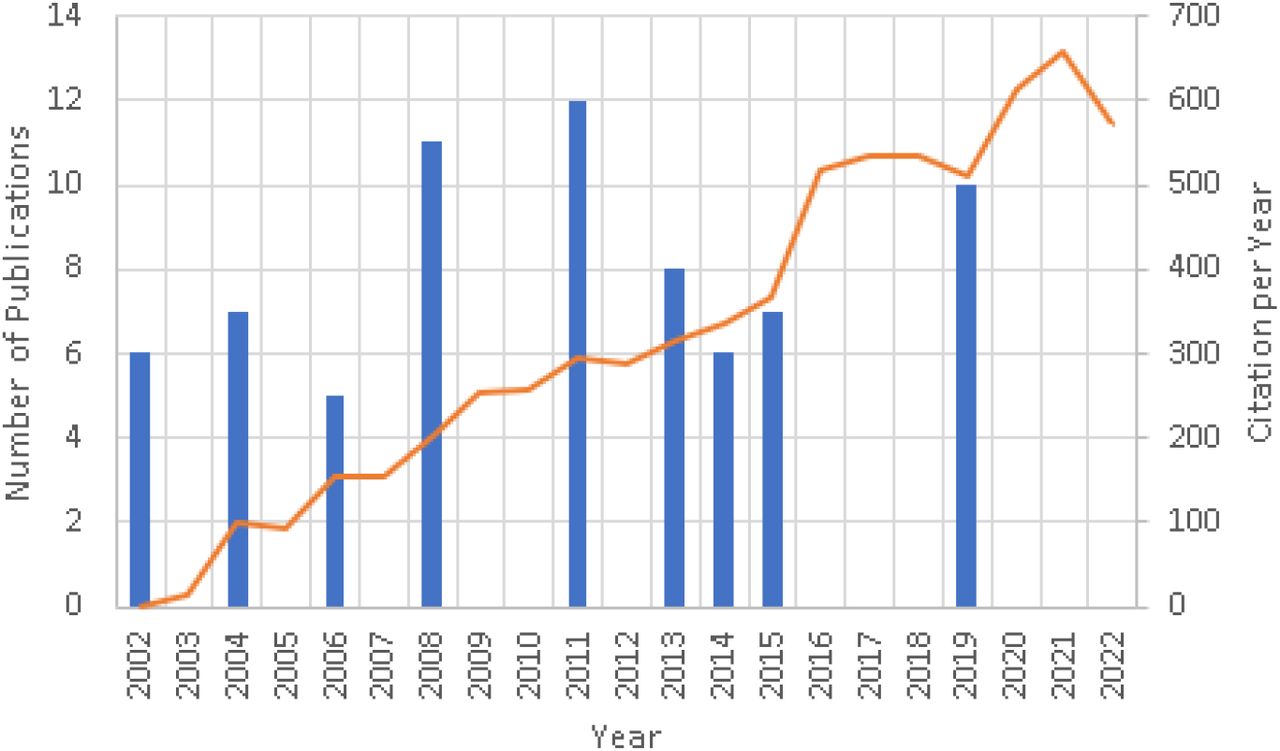
In total, there have been 10 conferences that resulted in 72 publications generated from 233 authors. See Table 1. From these publications, 5978 citations have been generated. Figure 1 is a summary of the number of citations per year for all PDC publications. In total 219 Adults, 28 FRAX-specific, and 41 Pediatric positions were found. In addition, there were 9 Nomenclature Positions discovered that are not specific to adults or children. To keep track of the positions and which ISCD document they are contained, a prefix was created where A=adult, F=FRAX, P=Pediatric and Nomenclature positions were given the prefix N. Executive summaries of the position statements from prior PDC’s held in 2001, 2003, 2005, 2007, 2010, 2013, 2015, 2019 have been published. 5,6,7,8,9,10,11,12,13,14,15

{kind=link}
2002 PDC: Denver Colorado (July 20-22, 2002) 5,16,17,18,19,20
This was the first ISCD PDC and generated six papers. The methods for developing positions were not yet standardized. The RAND method of Quality, Strength and Applicability, as was used at future conferences, had yet to be considered. The positions were presented in a narrative form in the executive summary and not summarized as position statements. This PDC addressed the most pressing questions of the time: Diagnosis of Osteoporosis by Central DXA Skeletal Sites 17, Osteoporosis Diagnosis in Males and Non-Caucasians 18, Serial BMD Measurements in Patient Management 19, and Peripheral Skeletal Site Measurements in Osteoporosis Diagnosis 20. These topics were considered pressing areas that needed clarification. Topics without controversy in the field were not addressed, but would be in future conferences.
2003 PDC: Cincinnati, Ohio (July 2003) 6,21,22,23,24,25,26
Like the first PDC, the methods for researching and forming positions had yet to be standardized. However, formal literature searches were performed with task forces. An expert panel reviewed the proposed positions, but no RAND criteria were followed especially for the grading of the position. This was the first PDC that summarized all ISCD positions in a comprehensive Executive Summary 21 organized into 15 categories. The 2003 PDC considered five categories for new positions including: the diagnosis of osteoporosis in men, premenopausal women, and children 23, technical standardization for dual-energy X-ray absorptiometry (DXA) 24, indications for bone densitometry 25, Reporting of bone density results, and nomenclature and decimal places for bone densitometry 26. There were now 98 bulletized positions from the society. Many of these were consolidated at later PDCs. Also at this PDC, the Canadian Panel of the ISCD issued an update to their standards of guidelines for performing DXA scans 27 that had been developed in coordination with the first PDC 28. These and subsequent works were regional interpretations of the official positions. Thus, the Canadian-specific and others similar works by regional societies were not included in the scope of the review.
2005 PDC: Vancouver, British Columbia, Canada (July 15–17, 2005) 7,29,30,31,32
Topics for consideration at 2005 PDC were developed by the ISCD Scientific Advisory Committee and the PDC Steering Committee. Specifically, these topics were the following: technical standardization, vertebral fracture assessment, application of the 1994 World Health Organization (WHO) classification to various skeletal sites, and application of the 1994 WHO classification to populations. It was the first time the positions addressed populations other than Caucasian women. The expert panel included representatives of the American Society for Bone and Mineral Research (ASBMR) and the International Osteoporosis Foundation (IOF), and the positions from this PDC were endorsed by both organizations. Endorsements like these were not always the case for previous and future PDCs. There was no substantive change in the format of the PDC or in its preparation from previous efforts.
2007 PDC: Lansdowne, Virginia (July 20–22, 2007) 8,33,34,1,35,36
For the 2007 PDC as the previous, the Expert Panel included representatives from other stakeholder societies including the ASBMR, the International Society for Bone and Mineral Research (IBMS) and the National Osteoporosis Foundation (NOF). Topics considered included vertebral fracture assessment, technical and clinical issues relevant to dual-energy X-ray absorptiometry (DXA), and bone densitometry technologies other than central DXA. This is the first PDC that began using a more formal approach to formulating the questions, refinement of the statements and appropriateness ratings using the RAND/UCLA Appropriate Method (RAM) 37. From this and subsequent PDCs, positions were rated for appropriateness, necessity, and quality of evidence as defined below.
Appropriateness
Statements that the Expert Panel rated as ‘‘appropriate without disagreement’’ according to predefined criteria derived from the RAM were referred to the ISCD BOD with a recommendation to become ISCD Official Positions (see below). A statement was defined as ‘‘appropriate’’ when the expected health benefit exceeded the expected negative consequences by a significant margin such that it was worth performing.
Necessity
Recommended Official Positions that were rated by the Expert Panel were then rated according to necessity to perform in all circumstances (see below), i.e., whether the health benefits outweighed the risks to such an extent that it must be offered to all patients. Necessity rating was conducted in a similar fashion as the appropriateness rating, in that each Official Position had to be rated as necessary without disagreement using similar predefined RAM criteria.
Quality of evidence
Good: Evidence includes consistent results from well-designed well-conducted studies in representative populations.
Fair: Evidence is sufficient to determine effects on outcomes, but the strength of the evidence is limited by the number, quality, or consistency of the individual studies.
Poor: Evidence is insufficient to assess the effects on outcomes because of limited number or power of studies, important flaws in their design or conduct, gaps in the chain of evidence, or lack of information.
Strength of recommendations
A: Strong recommendation supported by the evidence
B: Recommendation supported by the evidence
C: Recommendation supported primarily by expert opinion
Application of recommendations
W: Worldwide recommendation
L: Application of recommendation may vary according to local requirements
2007 Pediatric PDC: Montreal, Quebec, Canada (2007) 9,38,39,40,41
In 2007, ISCD convened its first Pediatric PDC to address issues specific to the assessment of skeletal health in children as young as 5 years, adolescents and adults below 20 years old since they were not explicitly included in previous positions. For this PDC, the Expert Panel included representatives of the ASBMR and IBMS. Before this pediatric conference, the positions developed were only directly applicable for adults without consideration of the appropriateness for children. Topics considered were included DXA prediction of fracture and definition of pediatric osteoporosis; DXA assessment in diseases that may affect the pediatric skeleton; DXA interpretation and reporting; and peripheral quantitative computed tomography measurement.
2010 PDC: Bucharest, Romania (November 14, 2010) 10,42,43,44,45,46,47,48,49,50,51,52
This PDC was jointly sponsored by the ISCD and the IOF to clarify a number of important issues pertaining to the interpretation and implementation of FRAX® in clinical practice. FRAX® (http://www.shef.ac.uk/FRAX) is a simple computer-based tool that integrates clinical information and femoral neck BMD as an option to predict the 10-year probability of major osteoporotic fracture and hip fracture 53. It has become the defacto fracture risk predictor used word-wide since it was developed from studying population-based cohorts from Europe, North America, Asia and Australia. The FRAX® algorithms give the 10-year probability of fracture. The output is a 10-year probability of hip fracture and the 10-year probability of a major osteoporotic fracture (clinical spine, forearm, hip or shoulder fracture). Yet, at the time of this PDC, the ISCD and IOF had no positions on how it should be incorporated into clinical practice.
2013 PDC: March 21–March 23, 2013 in Tampa, FL, USA 11,12,54,55,56,57,58,59
There have been many scientific advances in measurement of fat and lean body mass as determined by dual-energy X-ray absorptiometry (DXA). Previously, no guidelines to the use of DXA for body composition existed. The recommendations pertain to clinically relevant issues regarding DXA indications of use, acquisition, analysis, quality control, interpretation, and reporting were addressed. In addition, indications for DXA and vertebral fracture assessment and use of reference data to calculate bone mineral density T-scores were also updated. The Expert Panel included representatives of the IOF, the ASBMR, the NOF, Osteoporosis Canada, and the North American Menopause Society. The Task Forces included participants from 6 countries and a variety of interests including academic institutions, private clinics, and industry.
2013 Pediatric PDC: Baltimore, MD USA (October 2-3, 2013) 13,60,61,62,63,64
It had been 6 years since the last Pediatric PDC. The conference was co-sponsored by the ASBMR with the aim to focus on advances in the field since that initial conference that would lead to revisions of the original positions. The previous topics were revisited with the addition of recommendations for infants and young children.
2015 PDC: Chicago, IL, USA (February 26–28, 2015) 14,65,66,67,68,69,70
There have been many scientific advances in fracture risk prediction beyond bone density. This PDC was convened to address the use of beyond the measurement of bone mineral density for fracture risk assessment, including Trabecular Bone Score (TBS) and hip geometry measures. Previously, no guidelines for nonbone mineral density DXA measures existed. Furthermore, there had been advances in the analysis of quantitative computed tomography (QCT) and ISCD had no comprehensive positions on QCT. Task forces were asked to address these advances that included finite element analysis, QCT of the hip, DXA-equivalent hip measurements, and opportunistic screening.
2019 PDC: Kuala Lumpur, Malaysia (March 20-23, 2019) 15,71,72,73,74,75,76,77,78,79
This PDC was convened to both revisit previous positions including monitoring bone density change with DXA, DXA machine cross-calibration, and pediatric bone health, but also novel questions in smaller subspecialty areas where the ISCD had to date been silent including spinal cord injury, periprosthetic and orthopedic bone health, and transgender medicine.
ADULT POSITIONS BY CATEGORY
The adult positions are organized in a similar order and format as presented in the 2019 version of the Official Positions for Adults, Pediatrics and FRAX on the ISCD website and in the associated PDF version. In total, there are 43 categories.
1. Indications for Bone Mineral Density (BMD) Testing
Indications for BMD testing were first established at the 2003 PDC. Men under 70 years of age and women during the menopausal transition was added to the 2003 positions and both were then modified again at the 2013 PDC.
Position A1 regarding women 65 years and older wasn’t created in its current form until the 2003 25. It was created defacto at the 2001 PDC when the statement was made in Binkley et al. 18 that Caucasian and Non-Caucasian women should have the same indications, “The ISCD position is to apply existing indications for bone mass measurement in postmenopausal Caucasian women to non-Caucasian women. Thus, bone mass measurement is indicated for the following postmenopausal non-Caucasian women:
Those over age 65.
Those under age 65 with one or more risk factors.
Those with a prior fragility fracture
Those for whom knowledge of BMD would affect osteoporosis prevention/treatment decisions.”
This was resolved to make official positions for all race women at the 2005 PDC.
2. Reference Database for T-Scores
The use and calculation of T-scores has been addressed since 2001 at four separate PDCs. At the 2001 PDC, “there was insufficient data to definitively conclude that men and women fracture at the same DXA-measured BMD” 5. The question of what reference data to use for men and non-Caucasian populations has been examine multiple times since the first PDC. However, standardization to Caucasian females from the NHANES III for Femur Neck would not occur until 2005. Before that time, manufacturer specific reference data was common. In 2013, the conference examined if NHANES III should be used for spine as well. Ultimately, this proposal was turned down. See position A16.
3. Central DXA for Diagnosis
All of the positions in this section were finalized by the end of the 2005 PDC. However, there were critical updates to what sites were deemed valid for diagnosing osteoporosis during that time. Originally, trochanter was thought of as a valid diagnostic site. But trochanter was dropped at the 2005 PDC and 1/3rd distal femur was added if the spine and hip were both not valid. The current positions do not make mention which central DXA site is preferred for diagnosis and monitoring. However, the 2001 positions explicitly state that, “PA spine is the preferred site for monitoring. The total hip should be used when the PA spine is technically invalid.” These specific position statements were dropped in 2003.
4. Fracture Assessment
The presentation of these two positions in abstract of the controversies going on in the field obscures their meaning. A24 is stating that BMD can be used for both diagnostic classification of osteoporosis and quantifying fracture risk in fracture models. From the discussion in Hans 29, this was an important distinction at the time since diagnosis was being consolidated around one DXA measurement site, the femur neck, one reference database, NHANES III, and one T-score values of – 2.5. Simultaneously, it was being recognized that other technologies and regions of interests were still clinically important for other purposes, like monitoring change over time and quantifying fracture risk. These positions were trying to convey that it is OK to use one specific measurement for diagnosis and others for fracture risk. In the subsequent years, alternative technologies did not fair well in the marketplace, such as peripheral DXA, heel ultrasound, etc. and these distinctions became less important. But there is renewed interests in alternative technologies to DXA where these positions may again prove to be useful.
5. Use of the Term “Osteopenia”
These positions were created to encourage the use of “low bone mass” over osteopenia for interpreting T-score values. Osteopenia was often being thought of as a disease and ISCD wanted to discourage this. A full discussion can be found in Leslie et al. 30.
6. BMD Reporting in Postmenopausal Women and Men Age 50 and Older
These positions were to clarify the use of T- and Z-scores based on age and menopausal status, and the use of the WHO definitions of normal, osteopenia, osteoporosis, and established osteoporosis. Guidance on the specifics of how the T- and Z-score was to be calculated with respect to reference populations and race were covered in later positions.
7. BMD Reporting in Females Prior to Menopause and in Males Younger than Age 50
8. Z-Score Reference Database
9. Serial BMD Measurements
10. Phantom Scanning and Calibration
11. Precision Assessment
12. Cross Calibration of DXA: Changing Hardware or Systems
13. Cross Calibration of DXA: Adding Hardware or Systems
With lower reimbursement for DXA scanning at independent clinics in the US versus DXA scanning that takes place in medical centers 80, there has been a consolidation of DXA systems away from single system sites, to sites with multiple systems. The 2005 position was written in a language that implies that the need for cross-calibration was most likely due to replacing an older system with a new one. The 2019 positions are worded to address the needs of multi-system sites.
14. BMD Comparison Between Facilities
Although DXA quality control is a foundational principle for the ISCD, the comparison between facilities has only generated two positions. Since it is common for patients to move or to change health providers, this category of positions is of high interest. Yet, the positions themselves effectively state that DXA scans cannot be quantitatively and temporally followed if the patient is seen at more than one clinic. The author sees this as a failing in scope for the ISCD since this situation is so common.
15. Vertebral Fracture Assessment Nomenclature
Several other terms have previously been used for describing vertebral fractures from lateral DXA scans. Including morphometric X-ray absorptiometry (MXA), Instant Vertebral Assessment (IVA), Radiographic Vertebral Assessment (RVA), Lateral Vertebral Assessment (LVA), Dual-energy Vertebral Assessment (DVA) and others. Some of these terms were coined by specific DXA manufacturers. VFA was viewed by the expert panel of the 2005 PDC as a neutral term that the field could standardize around. See Vokes et al. 32 for the complete discussion.
16. Indications for VFA
The 2013 PDC greatly simplified the previous recommendations from 2005 and 2007 for greater ease of use and utilization by practitioners.
Original wording from 2007, “Postmenopausal women with low bone mass (osteopenia) by BMD criteria, PLUS any one of the following: Age greater than or equal to 70 yr, Historical height loss greater than 4 cm (1.6 in), Prospective height loss greater than 2 cm (0.8 in), Self-reported vertebral fracture (not previously documented), Two or more of the following: - Age 60 to 69 yr, - Self-reported prior non-vertebral fracture - Historical height loss of 2 to 4 cm, - Chronic systemic diseases associated with increased risk of vertebral fractures (for example, moderate to severe chronic obstructive pulmonary disorder (COPD) or chronic obstructive airways disease (COAD), seropositive rheumatoid arthritis, Crohn’s disease) (Grade: Fair-B-W-Necessary). Men with low bone mass (osteopenia) by BMD criteria, PLUS any one of the following: - Age 80 yr or older, - Historical height loss greater than 6 cm (2.4 in), - Prospective height loss greater than 3 cm (1.2 in) - Self-reported vertebral fracture (not previously documented), - Two or more of the following; - Age 70 to 79 yr, - Self-reported prior non-vertebral fracture, - Historical height loss of 3 to 6 cm, - On pharmacologic androgen deprivation therapy or following orchietomy, - Chronic systemic diseases associated with increased risk of vertebral fractures (for example, moderate to severe COPD or COAD, seropositive rheumatoid arthritis, Crohn’s disease) (Grade: Fair-C-W). Women or men on chronic glucocorticoid therapy (equivalent to 5 mg or more of prednisone daily for 3 mo or longer) (Grade: Fair-B-W-Necessary). Postmenopausal women or men with osteoporosis by BMD criteria, if documentation of one or more vertebral fractures will alter clinical management. (Grade: Good-C-W-Necessary)”
17. Methods for Defining and Reporting Fractures on VFA
One position was modified in 2007 from the 2005 positions on defining and reporting VFA. The changes drew upon an extensive literature search found in 33 such that the recommendation to use the Genant semiquantitative method were strengthened.
18. Indications for Following VFA with Another Imaging Modality
19. Serial Lateral Imaging
20. DXA to Detect Abnormalities in the Spectrum of AFF
Atypical femur fractures (AFF) are a type of fracture that occurs at the femur and is characterized by transverse or short oblique fractures with minimal or no trauma. Atypical femur fractures have been associated with the use of bisphosphonates, a class of drugs used to treat osteoporosis. 81
21. Baseline DXA Report: Minimum Requirements
These positions have not been updated in 20 years and most likely need revision to reflect the current needs of clinicians and patients.
22. Follow-Up DXA Report
These positions have not been updated in 20 years and most likely need revision to reflect the current needs of clinicians and patients.
23. DXA Report: Optional Items
This topic has not been addressed since 2013. There have been many updates in DXA systems since then. These positions are most likely in need of update to reflect the current technological capabilities.
24. DXA Report: Items that Should not be Included
25. Components of a VFA report
Vertebral Fracture Assessment (VFA) is a low radiation method for imaging the lateral spine for fracture assessment. The 2005 and 2007 PDCs addressed pressing issues regarding indications of use, methodology, and recommendations for additional imaging. One additional position on the use of serial VFA was also addressed in 2019, A95.
26. Trabecular Bone Score (TBS)
TBS is a proprietary measure of trabecular complexity in the spine. The 2015 and 2019 PDCs addressed the use of TBS but none of the existing positions were updated.
27. Hip Geometry
These positions are for hip geometry measures that may be useful for fracture risk assessment including hip axis length (HAL), cross-sectional area (CSA), Outer shaft diameter (OD), section modulus (SM), buckling ratio (BR), cross-sectional moment of inertia (CSMI), Neck Shaft Angle (NSA). Positions on their use were addressed at the 2015 PDC and not since.
28. General Recommendations for Non-Central DXA Devices: QCT, pQCT, QUS and pDXA
The following general recommendations for QCT, pQCT, QUS, and pDXA are analogous to those defined for central DXA technologies. Examples of technical differences among devices, fracture prediction ability for current manufacturers, and equivalence study requirements are provided in the full text documents printed in the Journal of Clinical Densitometry.
29. Baseline Non Central Devices (QCT, pQCT, QUS, pDXA) Report: Minimum Requirements
Three papers are listed for each of these reporting requirements since they are in common for each of the listed technologies and they have not been revised since their inception.
30. Non Central DXA Devices (QCT, pQCT, QUS, pDXA) Report: Optional Items
31. QCT and pQCT
Central quantitative computed tomography (QCT) of the spine and hip, and peripheral QCT (pQCT) have been addressed at the 2007 and 2015 PDCs. Further mention of CT is made in for orthopedic use in another section, see A241. Only one position, A173, has been updated. It addressed the situation when both QCT and DXA are available. The position was updated to state that DXA is preferred in this situation to limit radiation exposure.
32. QUS
Quantitative Ultrasound (QUS) systems were developed in the 1990s to evaluate fracture risk using the speed of sound (SOS) and/or broadband ultrasound attenuation (BUA). 82,83 Many regions on interest have been explored including the heel, proximal tibia, radius, phalanges, and recently the spine and hip. The use of QUS has only been addressed once at the 2007 PDC.
33. pDXA
Peripheral DXA (pDXA) systems are not as widely used in the US as central DXA systems, but still popular for bone evaluations by non-specialty providers (i.e. drug-store assessments) and in other countries. pDXA has only been addressed at the 2007 PDC.
34. Body Composition
Body composition by DXA has been available on DXA systems since 1987. However, there were no positions on indications for use, measurement, or reporting before the 2013 PDC. The topic has not been addressed since.
35. DXA in Patients with Spinal Cord Injury
Clinical care for patients with spinal cord injuries has been previously limited by the lack of consensus derived guidelines or standards regarding bone density testing and fracture risk prediction. No positions of the ISCD were directly applicable to those with spinal cord injury before the 2019 PDC.
36. DXA in Transgender and Gender Non-conforming individuals
All aspects of bone density testing in transgender and gender nonconforming (TGNC) individuals were poorly defined before the 2019 PDC.
37. Peri-prosthetic and orthopedic uses of DXA
Although the ability to measure bone surrounding metal protheses has been available for over 20 years, positions on the utility and reporting of peri-prosthetic bone was not addressed until 2019. The questions considered included, which orthopedic surgery patients should be evaluated for poor bone health prior to surgery, which subsets of patients are at high risk for poor bone health and adverse outcomes, what is the reliability and validity of using bone densitometry techniques and measurement of specific geometries around the hip and knee before and after arthroplasty was determined, how can CT be used to estimate bone quality at common orthopedic surgery sites.
FRAX POSITIONS BY CATEGORY
The FRAX calculator is a fracture risk assessment tool developed by the World Health Organization (WHO) 53. It is widely used to estimate the 10-year probability of a major osteoporotic fracture in an individual based on their age, sex, body mass index, other risk factors, bone mineral density and TBS score (if available). The FRAX calculator is used in clinical practice to identify patients who are at high risk for fragility fractures and who may benefit from preventive interventions. The FRAX statements are organized and numbered in the same fashion as found in the ISCD brochure. FRAX has only been addressed once by the ISCD, at the 2010 PDC. Thus, no edits are presented.
1. FRAX Introductory Statement
2. FRAX Clinical Statements
3. FRAX BMD Statements
4. FRAX International Statements
PEDIATRIC POSITIONS BY CATEGORY
Special considerations must be made when evaluating bone health in children. The size of the bone is a challenge to DXA systems since they were designed for larger adult bones. These positions were created to be exclusive to children without referral to the adult positions. Thus, some positions may seem similar to their adults counterparts.
1. Fracture Prediction and Definition of Osteoporosis
Fracture prediction and the definition of osteoporosis was first addressed at the 2007 Pediatric PDC. These positions were reviewed, and modifications were made to define significant fracture history and draw attention to the degree of trauma in fracture risk prediction. Extensive discussion can be found in Bishop et al. 63. The fracture risk statements are largely qualitative due to the lack of quantitative risk models in children.
2. DXA Assessment in Children and Adolescents with Disease that May Affect the Skeleton
Like other pediatric position categories, there has been substantial changes in the positions over the years. Three positions from the 2007 Pediatric PDC were removed from the ISCD positions in 2013. The removed positions are the following.
In patients with thalassemia major, spine and TBLH BMC and areal BMD should be performed at fracture presentation or age 10 yr, whichever is earlier (Fair-C-W);
Therapeutic interventions should not be instituted on the basis of a single DXA measurement (Fair-C-W);
When technically feasible, all patients should have spine and TBLH BMC and areal BMD measured before initiation of bone active treatment and to monitor bone-active treatment in conjunction with other clinical data (Poor-C-W).
In 2007, they were all based on expert opinion only (grade C) and in 2013 that expert opinion had changed in favor of removing the positions. The full discussion is beyond the scope of this review but can be found in Bianchi et al. 64.
3. DXA Interpretation and Reporting in Children and Adolescents
Reporting of densitometry for pediatrics has been under extensive revision since the 2007 PDC. The most dramatic changes in interpretation was with the proximal femur. See P11. This site was not originally recommended in 2007 primarily due to expert opinion regarding measures across the ever-changing mineralization around the growth plate of the greater trochanter. However, as evidence amassed, the proximal femur was found to be as precise as other bone regions and pediatric measurements would be useful for following an adolescent into adulthood. Further, many of the positions in this section were downgraded in their quality of evidence and strength of recommendation.
4. VFA in Pediatric Patients
The strengths and limitations of vertebral fracture assessment (VFA) by DXA were evaluated for use in children at the 2019 PDC. These positions are in response to the following questions: Should VFA be used as a substitute for spine radiography in the identification of symptomatic / asymptomatic osteoporotic VF in children? When does an abnormal VFA in a child require follow-up spine imaging? What is the VFA method that should be used to detect an osteoporotic VF in children? Are there technical and biological factors that limit the accuracy of DXA-based VFA in children (for example DXA model and software, age, sex, pubertal stage, obesity)? The full discussion of these questions and derivation of the positions can be found in Weber et al. 79.
5. pQCT in Children and Adolescents
There are currently three positions for pQCT and/or QCT for children listed by the ISCD on their website and all executive summaries since 2013. These three are the result of the 2013 Pediatric PDC. Two of these positions were updated positions from the 2007 Pediatric PDC. The change in wording is noted below the table. There are four additional positions from the 2007 Pediatric PDC that no longer appear in ISCD executive summaries or in their literature. These are listed as positions P34 -P37 and shown in italics. In discusssions with one of the surviving authors (Zemel), this omission is thought to be unintentional editorial deletions. Thus, they are included here and shown in italics. Adams et al. 62 provides a thorough presentation of the literature for studies using pQCT and QCT in children and adolescents.
6. Densitometry in Infants and Young Children
These are the only positions that directly address bone densitometry in Infants and children less than 5 years old. They were not included in the 2007 pediatric PDC. The primary paper, Kalkwarf et al. 61 offers not only justification for each position, but a comprehensive literature review for densitometry in young children. They found that there was insufficient information regarding methodology, reproducibility, and reference data to recommended forearm and femur measurements, and regarding to methods for accounting for growth delay as is done in older children Even though the positions document stated the positions were likely to be revisited as more data becomes available, they have not in the past 8 years most likely due to a continued lack of additional data.
NOMENCLATURE POSITIONS THAT APPLY TO ADULTS AND PEDIATRICS
1. DXA Nomenclature
These positions have only been discussed at the 2003 PDC and summarized in its executive summary (3). The positions were in response to a lack of consistency in reporting key DXA measures. These recommendations have been inconsistently followed in the literature especially in terms of labeling DXA as DEXA. For example, a Google Scholar search performed on 08/25/2021 for papers published in 2020 with either DXA or DEXA in the title found that 22 percent (38/169) of the titles used DEXA. The positions have not been modified since their inception and are broadly used. None of the positions were rated using the RAND criteria.
2. DXA Decimal Digits
Like DXA nomenclature, these positions have only been discussed at the 2003 PDC and summarized in its executive summary (3). The positions were in response to a lack of consistency in reporting quantitative measures. The positions have not been modified since their inception and are broadly used. None of the positions were rated using the RAND criteria.
DISCUSSION
Summary of evidence
This review has presented the context of the current 290 ISCD positions and provided a means to follow the etiology and pedigree of each position. The positions have been well utilized as evidenced by the over 6,700 cumulative citations to date. Their relevance is increasing as evidenced by the steady increase in annual citations. With over 230 authors participating in the writing and rationale for these positions, they are the most vetted and complete set of guidelines on the appropriate use of clinical densitometry. However, many positions have gone through extensive revisions while others have not been modified in over 20 years.
Before this scoping review, there was no single guide to the origins and rationale for the ISCD Positions. It could be argued that without this context, a clinician is blindly following an established paradigm without understanding of when, how and why it is appropriate.
Limitations
This scoping review, like all reviews, will be out of date as soon as it is published. But this is the nature of reviews. It is a snapshot of the field and its position at the time of this writing. Future researchers can hopefully use this as a starting point for updates after future PDCs. The review was also limited to the positions of the ISCD exclusively. There are positions for the use of DXA and guidelines for diagnosing osteoporosis from other organizations including the World Health Organization, National Osteoporosis Foundation and the International Osteoporosis Foundation. These were considered out of scope.
Conclusions
With 290 official positions, the ISCD has created one of the most complete and well documented set of recommendations for the use of DXA, QCT, pQCT and QUS to evaluate bone health in adults and children. This review links all source documents and wording changes to the current positions in the hope that it will be of use to those considering updates to the positions, and as an educational tool for those that seek a deeper understanding of how osteoporosis is managed and diagnosed. Updates to this review are warranted after each PDC.
Data Availability
All data generated produced for this review is contained in the manuscript
Funding
No funding was provided for this scoping review.
ACKNOWLEDGEMENTS
We appreciate the contributions from the following individuals: Geraldine Ragsac for her extensive research and copywriting.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵




