
Abstract
Background As cannabis legalization extends to numerous countries, encompassing both medicinal and recreational applications, understanding its impact on human body is crucial. The endocannabinoid (eCB) system, regulated by naturally occurring (endogenous) and externally derived (exogenous) cannabinoid compounds, plays a pivotal role in the host’s metabolism. This system, in conjunction with the host’s immunomodulatory mechanisms, influences the composition of the gut microbiota, resulting in beneficial outcomes for the gastrointestinal (GI) and immunological systems.
Objective This systematic review aims to evaluate the association between cannabis treatment and the gut and oral microbiome, supporting further clinical trials in this area.
Methods A comprehensive literature search was conducted on online platforms such as PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library. The search encompassed studies published until July 20, 2022, focusing on adult populations with clinical abnormalities. Only English language studies were included. Identified studies were analyzed, considering predetermined subgroups based on different disease conditions. A random-effects meta-analysis was employed to qualitatively and quantitatively combined and assess the data.
Result The study comprised 9 studies with 2526 participants, including 2 clinical trials and several observational studies. The research explored the impact of marijuana (MJ) use on the microbiota across various clinical categories, such as HIV infection, pain/inflammation, systemic aspergillosis, obesity, cognitive deficits, and oral diseases. Qualitative analysis of the included studies revealed diverse and condition-specific effects of MJ use on the microbiota, such as decreased microbial diversity and increased cannabinoid excretion.
Conclusion These findings shed light on the complex effects of cannabis use on the human microbiota, underscoring the need for furture research on the therapeutic potential of cannabis. This review provides valuable insights to guide future investigations in this field.
Funding None

Short Summary With the global expansion of cannabis legalization, understanding the effects of cannabis on the human body, particularly among individuals with diverse clinical conditions, is of paramount importance. Through a meticulous systematic review utilizing comprehensive data, our findings uncover that cannabis consumption in adults with varied clinical conditions leads to discernable alterations in the human microbiome. These noteworthy modifications necessitate careful consideration in future investigations exploring the potential beneficial or adverse effects of cannabis treatment on patients.
Introduction
Marijuana (MJ), or Cannabis sativa, has a long history of use both for therapeutic and recreational purposes. It can also be called cannabis, weed, pot, or dope; all refer to the dried flowers, leaves, stems, and seeds of the cannabis plant (1). The chemical constituents the cannabis consist of a complex mixture of natural cannabinoids containing approximately 500 bioactive detected compounds with 70 different cannabinoids (2). Cannabidiol (CBD), a non-psychoactive cannabinoid molecule, had its chemical structure first determined in 1963, and the psychoactive cannabinoid, δ9-tetrahydrocannabinol (THC), was then discovered in 1964 (3). People use it in various ways, including via smoking, inhaling, and as cannabis extracts.
After alcohol and cigarettes, cannabis is the drug that is used most frequently for psychoactive purposes globally (4). In 2020, the global cannabis user population was over 4%, and nearly 6% among ages (5). Even though there is little evidence that adult patients consume cannabis, its consumption in older populations aged ≥ 50 years has been elevated from 15.1% in 2014 to 23.6% in 2016 since legalization for medical use encouraged former non-users to start using it (6). In the United States, the utilization of cannabis is increasing for medical and recreational purposes while the potential risk is declining (7, 8, 9). Even though there is little knowledge of the dangers and advantages of it, they primarily utilize it to control the symptoms.
The endocannabinoid system (ECS) is a ubiquitous modulatory neurotransmission system in the brain, and it consists of endogenous neurotransmitters (also known as endocannabinoids (eCBs)) derived from fatty acids, the enzymes responsible for their breakdown, and cannabinoid receptors (CBRs) to which endogenous and exogenous, plant-based cannabinoids bind (10). Nearly all the effects of cannabinoids are mediated by CB1 and CB2 receptors, which are predominantly expressed in the brain and immune cells, respectively (11, 12, 13).
Cannabinoids have a well-established, proven record as anti-inflammatory drugs with many immunosuppressive characteristics (14). It was shown that CBD stimulated myeloid-derived suppressor cells (MDSCs), which inhibited T cell proliferation in vitro and in vivo (15). It has also been demonstrated that THC can stimulate MDSCs without using toll-like receptor 4 (TLR4) and then stimulates regulatory T cells (Tregs) that play a role in their differentiation and functions and secrete immunosuppressive cytokines such as interleukin-10 (IL-10) and transforming growth factor β (TGF-β) (16, 17).
While increasing the legalized countries for cannabis use, more research studies are being explored on its potential therapeutic effects and adverse outcomes. Cross-sectional research of primary care patients indicated that those who use medical cannabis have more possible advantages than those who don’t, but there are still adverse effects (18). From a systematic review of randomized clinical trials (RCTs) of medical cannabinoids, the serious adverse events are categorized into respiratory, thoracic, and mediastinal disorders, GI disorders, nervous system disorders, cerebrovascular disorders, general disorders and administration-site conditions, renal and urinary disorders, neoplasm, psychiatric disorders and others (19). Furthermore, it is evident that the most frequent physical health reasons are to manage pain (53%), sleep (46%), headaches/migraines (35%), appetite (22%), and nausea/vomiting (21%), while the most prevalent mental health reasons are anxiety (52%), depression (40%), and PTSD/trauma (17%) (20).
A mutually beneficial symbiotic interaction exists between the host and the diverse GI microbial population that can be found here (21). The gut microbiota plays a significant role in host metabolism and is associated with the regulation of the inflammatory status of the host in the gut but is not limited to other organs like the brain (22). The intestinal microbiota affects neurological, endocrine, and immunological networks through the gut-brain axis and the bilateral communication between the central and enteric nerve systems (23, 24). A recent study reveals that the gut microbiome plays a role in anxiety and depression-like behavior (25), and clinical research indicates that these disease situations are characterized by an abundance of pro-inflammatory and short-chain fatty acid (SCFA) producing bacterial species (26). This pathophysiology illustrates that dysbiosis may have positive or negative consequences on the host’s inflammatory condition.
The positive effects of cannabinoids on the GI and immunological systems are lowering intestinal permeability, controlling intestinal bacteria, and reducing inflammation, according to earlier preclinical studies (27, 28). Numerous active studies on cannabinoids in the field of natural medicines are underway at the moment since there is evidence to support their potential efficacy in treating cardiovascular disease, cancer, and inflammation (29, 30, 31, 32). On the other hand, it was linked to detrimental impacts on both physical and mental health in a dose-response manner, with daily or nearly daily use being linked to worse results (33).
The gut-brain axis and bacterial metabolites and products have recently come to light as a mechanism by which intestinal bacteria can influence the physiology and inflammation of the central nervous system (CNS) (34). These mechanisms are dysregulated and then linked to altered blood-brain barrier (BBB) permeability and neuroinflammation during dysbiosis (34). A. muciniphila, one of the numerous bacterial species in the gut, significantly regulates the gut barrier and processes roughly 3–5% of the gut microbiota in healthy humans (35, 36). The regulation of intestinal barrier integrity, effects on immunological modulation and the enteroendocrine system, and mediators from the microbiome entering the body could all be implicated in this process.
The amount of eCBs linked to alterations in Peptostreptococcaceae, Veillonellaceae, and Akkermansiaceae has been found to elevate in response to dietary treatments using certain fatty acids (37). In addition to enhancing the quality of life (QoL), cannabis use can affect eCB tone and promote mucosal healing in people with ulcerative colitis (UC) (38). It has also been documented to favor immune suppression in vivo through the modulation of the eCB system using cannabinoids (39).
In a mouse model of Staphylococcal enterotoxin B (SEB)-induced acute respiratory distress syndrome (ARDS), AEA treatment increased the abundance of beneficial bacteria producing SCFAs like butyrate as well as production of antimicrobial peptides (AMPs) and tight junction proteins (TJPs), which are essential molecules sustaining epithelial barrier integrity in lung epithelial cells and decreased the pathogenic Enterobacteriaceae and Pseudomonas (39). While examining the effectiveness of THC therapies, Ruminococcus gnavus, a good bacterium, was discovered to be more prevalent and pathogenic A. muciniphila in the gut and lungs was decreased along with the enrichment of propionic acid (40). Another mouse study found that combining THC and CBD reduced the signs of experimental autoimmune encephalomyelitis (EAE), which was characterized by an increase in anti-inflammatory cytokine production, a decline in pro-inflammatory cytokines, a reduction in mucin-degrading A. muciniphila, and a reversal of the high level of lipid polysaccharides (LPS) (41). Collectively, these findings indicate that cannabis affects the gut microbiome.
There is growing evidence that cannabis may promote healthy gut flora, communication between the gut and the brain, and overall robust gut health (10, 42). Cannabinoids can interact with their receptors in the gut, and it has been used for hundreds of years to treat the symptoms of inflammation and GI diseases, such as abdominal discomfort, cramps, diarrhea, nausea, and vomiting (43). Hence, the systematic review would be the first to evaluate several observational studies in human and clinical trials using marijuana to alter the microbiota to treat various diseases, hoping to encourage additional thorough research studies.
Materials and Methods
Protocol and registration
The systematic literature review was registered on PROSPERO ID 2022 CRD42022354331.
Literature search
According to the PRISMA declaration guidelines, a thorough literature review and meta-analysis were undertaken (44). The study’s inclusion and exclusion criteria were developed using the PICO/PECOs methodology (45, 46). Four authors (MT, TO, SH, and AJ) independently assessed each study for eligibility in the systematic review by examining PubMed, Embase, and Cochrane databases. Any discrepancies were resolved through group discussions at each stage. The search was explicitly focused on cannabinoids and microbiome-related studies conducted in the English language. Studies that exclusively involved animals or lacked peer review were excluded. These databases encompassed epidemiological and intervention research, explicitly emphasizing the effects of cannabis treatment and its impact on the microbiome. The data extracted for analysis included studies published until July 20, 2022.
Study selection
Before conducting full-text reviews, two reviewers (MT, TO, SH, and AJ) independently assessed papers to determine their suitability based on predetermined inclusion and exclusion criteria. Full-text versions of all relevant documents were obtained for further data extraction. The inclusion criteria for the meta-analysis encompassed interventions investigating the effects of any cannabis treatment and its impact on microbiome modification, with or without active or placebo controls. The following publications were excluded: animal studies, in vitro research, review articles, protocols, letters, editorials, comments, suggestions, and guidelines. Any disagreements among the authors were resolved through consensus.
Data extraction
Independent reviewers (MT, TO, SH, and AJ) conducted the data extraction process and collected information on various variables. These variables included 1) study characteristics such as author names, publication year, study period, study type, country, sample size, and age range; 2) baseline characteristics of the included studies, encompassing participant information, study region, and clinical conditions reported by both patients and controls; 3) subgroup evidence categorized by specific diagnostic health problems; and 4) adverse reactions associated with the consumption of MJ—the data extraction involved thoroughly examining relevant text, tables, and figures. In the case of any discrepancies between the reviewers, they were resolved through discussion or reaching a mutual agreement.
Risk of bias
The evaluation of the risk of bias (ROB) in the extracted intervention study (47) was carried out by two independent authors (MT, TO, SH, and AJ). In the case of non-randomized clinical trials (48), the ROB was assessed using the ROBINS-I (Risk Of Bias In Non-randomized Studies -of Interventions) tool (49). For cohort and case-control studies that were included (50, 51, 52, 53, 54, 55, 56), the two authors independently assessed the ROB using the Newcastle-Ottawa Quality Assessment Scale (NOS) (57).
Statistical analysis
The prevalence of the baseline characteristics was described by total number and percentage by group. The overall mean age of included studies was calculated using combined mean and standard deviation (SD) techniques. For outcomes related to microbiome diversity in intervention trials, mean differences (MD) and a 95% confidence interval (95% CI) between groups were provided. The clinical and methodological variability of participant characteristics, study time, study type, and study site were also evaluated qualitatively.
Results
Study selection
In the initial literature search, 4,022 articles were identified across various databases. After removing 1,222 duplicates, the titles and abstracts of the remaining 2,800 studies were analyzed. Based on the predetermined inclusion and exclusion criteria, 2,766 publications were excluded. The remaining 30 articles underwent full-text screening to determine their eligibility for inclusion in the systematic review. Of these, 21 studies were disqualified for the following reasons: one editorial, one letter to the editor, one protocol, six studies with incorrect study designs, and twelve non-peer-reviewed studies. Ultimately, the systematic literature review included 9 studies that met the eligibility criteria (Figure 1).

Flow diagram for identifying studies in the systematic literature review. Across different databases, 4,022 articles were identified, but 1,222 duplicates were removed at the initial identification step. After the abstract and full-text screening, only 9 out of the initial pool of 2800 studies were included in the systematic review.
Study characteristics
Among the included studies were one case-control study (54), six cohort studies, and two clinical trials (47, 48). These studies involved 2,526 participants and covered a research period ranging from 1983 to 2021, as indicated in Table 1. The data for these studies were collected from four different countries: the United States of America (USA), the Islamic Republic of Iran (Iran), the State of Israel, and the United Kingdom (UK). The study durations varied, ranging from 1 to 3 years. The age range of the study population spanned from 17 to 101 years.
Subject characteristics
We discovered that 43% of participants played a role as patients, whose ages ranged from 17 to 101, as opposed to control groups, whose ages ranged from 18 to 87. The controls had a lower mean age of 28.4 years, whereas the patients’ average age was 56.5 years. Women comprise more than 85% of the participants, with the USA contributing the most. Patients are more likely to suffer cognitive impairment (76.6%) than HIV infection cases (11.1%) and others (Table 2).
Risk of bias
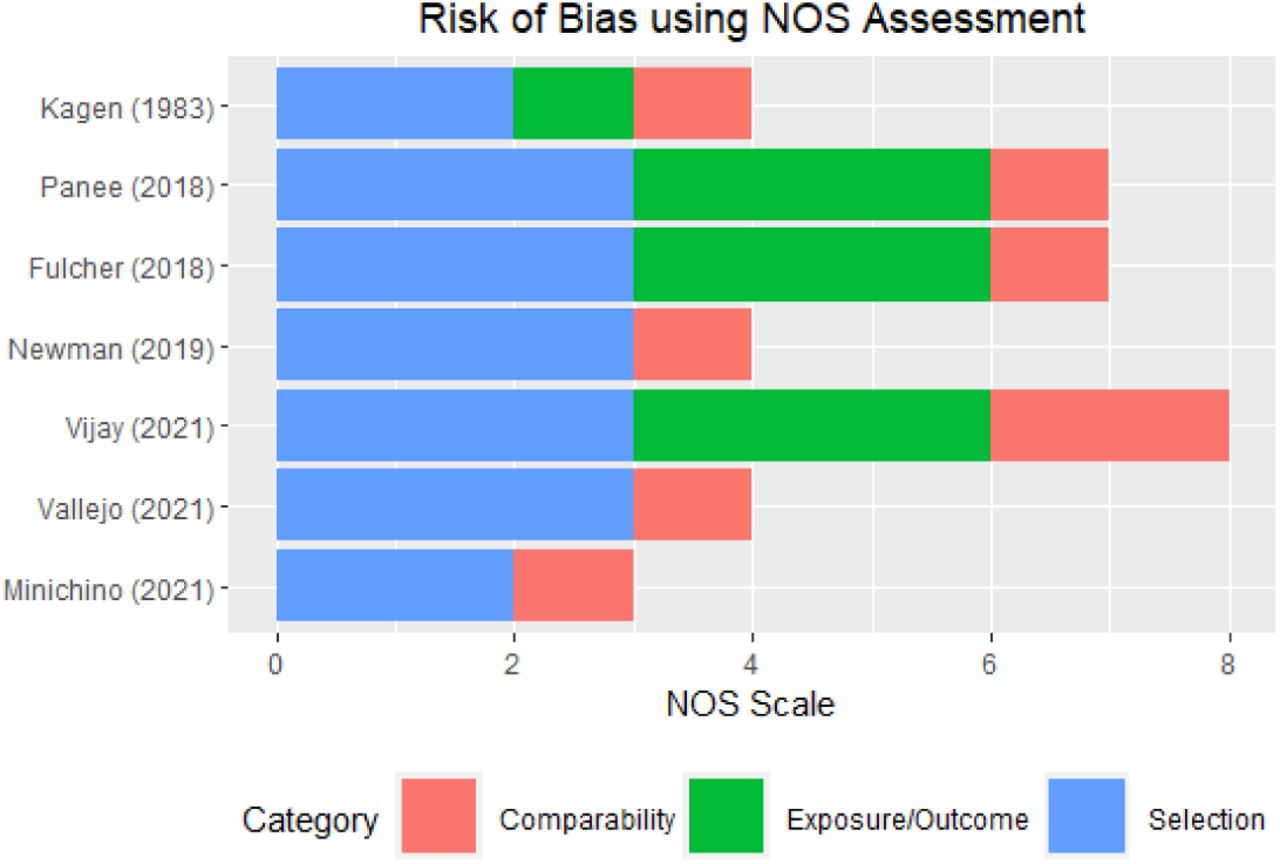
The review comprised 7 observational studies (50, 51, 52, 53, 54, 55, 56) assessed for the ROB using the NOS assessment technique (Figure 2). Among these studies, only one conducted by Minichino et al. displayed a very high risk of biases. This was due to the absence of a description of the non-exposed cohort, the inability to blind the outcome assessors, and a lack of follow-up information. Similarly, previous cohort studies by Newman et al., and Vallejo et al. also exhibited biases due to challenges in outcome assessment blinding and the absence of a follow-up timeline description. In the case-control study by Kagen et al., a significant bias was identified due to a lack of statements regarding case and control selection and exposure.

Assessment of risk of bias for cohort and case-control studies using the NOS assessment tool
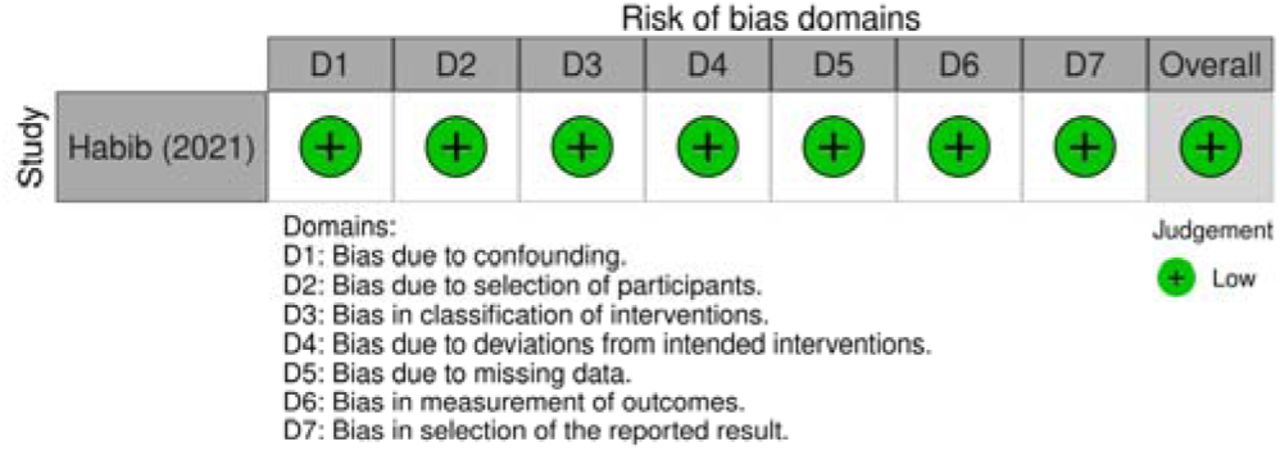
Furthermore, in the reported results of the RCT conducted by Payahoo et al., there was evidence of selection bias as they did not include the specified lipid profile analysis mentioned in their protocol (Figure 3). On the other hand, the non-RCT study conducted by Habib et al. demonstrated a well-performed risk assessment (Figure 4).

Assessment of risk of bias for randomized controlled trials

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Assessment of risk of bias for non-randomized controlled trials
Microbiota alteration by different cannabis usage
We conducted a qualitative analysis of the alterations in microbiota observed in patients with various clinical conditions when using MJ/medical cannabis and its compounds. This analysis also encompassed the examination of microbial diversity and factors associated with these changes, as presented in Table 3.
Adverse events
Six patients (21.4%) reported symptoms, including coughing and wheezing after using MJ cigarettes, while one (3.5%) suffered drowsiness, night sweats, systemic aspergillosis, and coughing bouts. Steven et al. reported these negative consequences, which went away quickly after quitting smoking MJ (54).
Discussion
The comprehensive study supported the link between cannabis usage and microbiota in a variety of patients suffering from oral illness, obesity, systemic aspergillosis, pain/inflammation, and HIV infection. The utilization of MJ was performed by substance use, oral capsules, or cigarette smoking.
Microbial alteration in HIV patients using MJ
Approximately 77% of HIV patients were lifetime MJ users, while the proportion of uninfected counterparts was 44.5% in a nationally representative sample (58). Research in this area suggests that cannabinoids are anti-inflammatory in the setting of HIV through the effect of ECS in the gut and through stabilization of gut-blood barrier integrity (59).
Fulcher et al. conducted a study focusing on HIV-positive men who have sex with men to examine the impact of MJ usage on gut microbiota (52). The study consisted of two visits with a 6-month interval, during which 49% of participants reported MJ use on the first visit, and 30% reported MJ use on the second visit. Utilizing permutational multivariate analysis of variance, the study revealed a positive correlation between MJ use in HIV patients and an increase in Fusobacterium and Anaerotruncus, as well as a negative association with the abundance of Dorea organisms (52), as indicated in Table 3.
Typically, MJ users in HIV patients engage in higher-risk sexual conduct or practices leading to bacterial vaginosis (BV), characterized by lacking Lactobacilli and the overgrowth of facultative anaerobic organisms (55). Furthermore, the prevalence of trichomonas infection in rectal samples decreased from 14% to 5% over the 6 months (p=0.08), while gonorrhea and syphilis infections increased from 8% to 11% (p=0.66) and 0% to 5% (p=0.16), respectively (52). On the contrary, a prospective study showed that the patients using marijuana were more than six times as likely to test positive for T. vaginalis (aOR=6.2, p=0.0003) (60). Additional clinical studies are needed to address the ongoing controversy surrounding the association between marijuana use and changes in sexually transmitted diseases.
Vallejo et al. conducted a cohort study focusing on females of reproductive age who experienced vaginal discharge (55). Out of the participants, 15% reported marijuana (MJ) usage. Among those with recurrent bacterial vaginosis (BV), 28.7% (23 out of 80 patients) were MJ users, while among those without recurrent BV, 14.2% (185 out of 1300 patients) reported MJ usage (p<0.01). Logistic regression analysis indicated a significant association between MJ use and recurrent BV, with an adjusted odds ratio of 2.05, as presented in Table 3.
Interestingly, Fulcher et al. also found that 28.4% of the MJ users have a history of asthma patients while 18.3% of the non-users (p<0.01) (52). Since cannabis has a bronchodilator effect on the airway, it has beneficial effects for asthma patients, yet, there are some detrimental effects on the lungs (61). With reported improvement in asthma symptoms, it might be used for medicinal or recreational purposes.
Impact of MJ on microbiota regarding pain or inflammation
To investigate the functional interactions between the eCB system and the gut microbiome in regulating inflammatory markers, Vijay et al. conducted a 6-week exercise intervention (50). They discovered that changes in anandamide (AEA) were positively associated with butyrate, and increases in AEA and palmitoylethanolamide (PEA) were correlated with decreases in TNF-α and IL-6. These associations statistically mediated one-third of the effect of short-chain fatty acids (SCFAs) on these cytokines (50). The findings suggest that the eCB system plays a role in the anti-inflammatory actions of SCFAs, indicating the involvement of additional pathways in the regulation of the immune system by the gut microbiota. Therefore, improved EC tone induced by exercise may mediate the shift in the gut microbiota to increased SCFA producers, thereby increasing the SCFA production without a dietary change.
Musculoskeletal pain is the most common cause of chronic non-cancer pain, and the perceptions of these patients are that cannabis can help to relieve the pain with only minor adverse effects and improve psychological well-being (62). In a clinical trial on patients with musculoskeletal pain using medical cannabis treatment, it found an elevation of S. mutan and Lactobacilli in 4th week even though the first was low at the first week (48). It was unexpected to see levels of S. mutans or Lactobacilli rise afterward. It is possible that cannabis either had a favorable or unfavorable effect on these particular bacteria, promoting the growth of these two oral bacteria.
Different expression of microbiota in oral diseases after the use of MJ
Newman et al. found that genera earlier shown to be enriched on head and neck squamous cell carcinoma (HNSCC) mucosa, such as Capnocytophaga, Fusobacterium, and Porphyromonas, were at low levels at the tongue site in MJ users, while Rothia, which is found at depressed levels on HNSCC mucosa, was high (56). At the oral pharynx site, differences in bacteria were distinct, with higher levels of Selenomonas and lower levels of Streptococcus, as seen in HNSCC. In samples taken from the lateral border of the tongue and the oral pharynx, which are both different when it comes to the MJ-linked microbiome, it was found that daily/almost daily inhalation of MJ over the previous month correlates with differently abundant taxa of the oral microbiome. The use of MJ is associated with changes in bacteria levels, but it has not been established that it is the cause of how normal tissue develops into disease and then SCC. Furthermore, these changes were not consistent with malignancy. Lateral tongue sites demonstrated microbiological changes with MJ usage.
Gut microbiota in cognitive deficits with the use of MJ
Moreover, using MJ is associated with alterations in gut microbiota and mitochondrial (mt) function, leading to further cognitive deficits (51). It was associated with lower fruit and vegetable consumption and greater animal-based food consumption in adults and adolescents. It also found that a more extensive lifetime MJ use was associated with a lower Prevotella: Bacteriodes ratio, as indicated in Table 3. The authors suggested that MJ use and associated dietary change contribute to microbiome alteration along with lower dietary intake of antioxidants and fibers.
Effect of cannabinoids in obesity in terms of microbiome
Obesity is an excessive buildup of fat that can be unhealthy for health and cause an inflammatory response (63). Currently, herbal remedies are gaining popularity in the treatment of obesity and its co-morbidities, and Cannabis sativa derivatives are receiving much attention. In the randomized double-blind controlled clinical trial, it was discovered that energy intake, fat, protein, and carbohydrate declined significantly (p<0.001) in the OEA group (47). OEA supplement use significantly decreased the energy and carbohydrate intake of obese participants, and A. muciniphila bacterium increased considerably in the OEA group compared to the placebo group, suggesting that OEA could be used as a supplement for obese people (62).
Dysbiosis in cognitive deficits using MJ
Both mitochondrial (mt) dysfunction and gut dysbiosis also affect cognition. From the preliminary findings from Panee et al. (51), mt function correlated positively with Fluid Cognition and Flanker Inhibitory Control and Attention scores in MJ users but not in non-users (interaction p=0.0018–0.08).
Conclusion
Our goal was to compile a comprehensive picture of the microbiome associated with MJ use. In the systematic review, it was reported that both the ECS and the GI microbiota could individually contribute to the manifestation of pain and others. Despite the limited literature dedicated to these interactions to date, this should be anticipated for further work in this exciting research field.
Data Availability
All data produced in the present work are contained in the manuscript as supplementary files.
Authors’ contributions
MT and SR contributed to the analysis and writing of the manuscript. MT, TO, SR and KP contributed to the conception and design. MT, SR, and AJ conducted the data curation. MT, TN, NH, and KP contributed to the critical revision of the manuscript. All authors read and approved the final manuscript. KP is the guarantor of the review.
Funding
M.T. was supported by the Graduate Scholarship Programme for ASEAN or Non-ASEAN Countries, Chulalongkorn University. T.O. and K.P. were funded by the Second Century Fund (C2F), Chulalongkorn University.
Availability of data and materials
Data will be available as supplementary files.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Acknowledgments
None
Footnotes
mst.maysoethu{at}gmail.com, thunnichaon{at}yahoo.com, szayehall01{at}outlook.com, tnopsopon{at}gmail.com, ananyajagota{at}gmail.com, nattiyap{at}gmail.com
Study title changed; Abstract revised; Content updated.
Abbreviations
- CENTRAL
- Cochrane Central Register of Controlled Trials
- CIs
- Confidence intervals
- GRADE
- Grading of Recommendation Assessment, Development and Evaluation
- NOS
- Newcastle - Ottawa Quality Assessment Scale
- PRISMA-P
- Preferred Reporting Items for Systematic review and Meta-analysis Protocols
- RCTs
- Randomized controlled trials
- ROBINS-I
- Risk Of Bias In Non-randomized Studies - of Interventions
- US
- United States
References



