
Abstract
Paenibacillus thiaminolyticus may be an underdiagnosed cause of neonatal sepsis. We prospectively enrolled a cohort of 800 neonates presenting with a clinical diagnosis of sepsis at two Ugandan hospitals. Quantitative polymerase chain reaction specific to P. thiaminolyticus and to the Paenibacillus genus were performed on the blood and cerebrospinal fluid (CSF) of 631 neonates who had both specimen types available. Neonates with virus detected in either specimen type were considered to potentially have paenibacilliosis, (37/631, 6%). We described antenatal, perinatal, and neonatal characteristics, presenting signs, and 12-month developmental outcomes for neonates with paenibacillosis vs. clinical sepsis. Median age at presentation was 3 (interquartile range 1, 7) days. Fever (92%), irritability (84%) and seizures (51%) were common. Eleven (30%) had an adverse outcome: 5 (14%) neonates died during the first year of life; 5 of 32 (16%) survivors developed postinfectious hydrocephalus and one (3%) additional survivor had neurodevelopmental impairment without hydrocephalus. These results highlight the need to consider local pathogen prevalence and the possibility of unusual pathogens when determining antibiotic choice for neonatal sepsis.
Neonatal sepsis is a leading cause of early childhood death worldwide.1,2 Affected infants are disproportionately from low-resource settings.2 Survivors of neonatal sepsis have an increased risk of neurodevelopmental impairment3,4, hydrocephalus5 and cerebral palsy.6 Effective antibiotic therapy relies on identification of the causative pathogen or, in the absence of this information, empirical therapy that is broad enough to provide effective coverage of the most likely pathogens.6
In low-resource settings, blood and cerebrospinal fluid cultures are often unavailable or uninformative.7 Cultures can be negative for a variety of reasons including low sample volume and technical limitations.8 Some pathogens are unculturable or are difficult to culture using routine culture methods. Culture-independent methods to identify causative pathogens have recently become possible due to advances in molecular diagnostics. Because of their cost and technical requirements, these methods are not widely available and have only rarely been used to identify pathogens affecting neonates in low-resource settings.9,10
Current international guidelines recommend the combination of ampicillin and gentamicin as first-line empirical antibiotic therapy for neonates with sepsis.11 However, in regions where antibiotic resistance is common, these antibiotics are not the ideal treatment for many neonatal infections.12-14 Without local culture and antibiotic susceptibility testing, the risk of antibiotic resistance is unknown; in these cases, ampicillin and gentamicin may be inadequate treatment. 15,16,15,16,15,16,15,16,15,16
In previous work, using targeted metagenomics, we found 41% of infants with postinfectious hydrocephalus, a common sequela of NS in Uganda, had a Paenibacillus spp infection.15,17 We sought to describe the clinical syndrome of neonatal Paenibacillus infection among Ugandan neonates presenting with clinical signs of sepsis, to report 12-month outcomes for infants with this novel infection and to compare patient characteristic and outcomes for infants with Paenibacillus infection compared to infants with clinical sepsis without Paenibacillus detected. We hypothesized that infants with Paenibacillus detected would be more likely to have the composite outcome of postinfectious hydrocephalus, death or neurodevelopmental impairment than those without Paenibacillus detected.
Methods
Study Population
Ugandan neonates (≤ 28 days of age) previously enrolled in a parent study were evaluated for inclusion in this subanalysis focused on Paenibacillus infection. The parent study enrolled 800 neonates presenting to two regional referral hospitals with clinical signs of neonatal sepsis (fever, poor feeding and lethargy; hypothermia, poor feeding, and lethargy; seizures and/or bulging fontanelle, poor feeding, and fever) were recruited. The study sites were, Mbale Regional Referral Hospital in Eastern Uganda, and Mbarara Regional Referral Hospital in Western Uganda. Neonates born at a gestational age < 37 weeks or < 2000 grams birthweight, and those who had been diagnosed with birth asphyxia or hypoxic ischemic encephalopathy were excluded. Following informed written consent, blood and cerebrospinal fluid were collected from each neonate using aseptic technique. Infants were eligible for this subanalysis if they had sufficient blood and CSF to perform qPCR for Paenibacillus genus and P. thiaminolyticus (N=631).
Laboratory Analysis
An aliquot of each was collected into DNA/RNA preservative (DNA/RNA Shield, Zymo Corporation) and frozen at -80° C. Additional aliquots of blood and CSF were processed in the local clinical laboratory for standard-of-care clinical tests. Once the entire cohort had been enrolled, the frozen samples were transferred to Penn State University for processing. CSF was available for 631/800 (79%) of the neonates enrolled. For these 631, we performed quantitative polymerase chain reaction (qPCR) on the blood and CSF using primers specific to both the Paenibacillus genus and P. thiaminolyticus. Neonates with detection of virus using either test were considered to have possible paenibacilliosis.
Demographics, birth history, clinical signs at presentation and during the hospital stay, results of laboratory tests performed as part of clinical care and antibiotics administered were abstracted from each infant’s medical record. In Uganda, current clinical guidelines recommend that the umbilical cord stump receive no care (dry cord care) or be cleansed with chlorhexidine (Umbigel™). Mothers were asked to indicate how they cared for the neonate’s cord stump at home including any substances applied to the cord stump prior to presentation. The presence of seizure-like movements was considered to represent seizures; no electroencephalograms were performed. Fever was defined as a temperature ≥38° C.
Infants underwent developmental assessments at 2 months, 6 months and 12 months of age using the Bayley Scales of Infant and Toddler Development Third Edition (BSID-III).18 Population-normalized BSID-III scores range from 1 to 19 with a population mean of 10, and a standard deviation (SD) of 3. Neurodevelopmental impairment (NDI) was defined as a BSID-III score < -2SD on any of the subscales.
We compared the demographic characteristics, presenting clinical signs, antibiotic treatment and clinical course for patients with neonatal paenibacillosis to septic neonates without P. thiaminolyticus detected using Fisher’s exact test for proportions and Wilcoxon rank-sum test for continuous variables. Similarly, we compared the proportion of patients with and without paenibacilliosis who experienced in-patient death, infant death (death between birth and 1 year of age), postinfectious hydrocephalus (PIH), NDI, and the composite of infant death, PIH or NDI during the first 12 months of age using Fisher’s exact test. Finally, for infants with paenibacilliosis, we compared the proportion of patients with fever, irritability, seizure, tachypnea, respiratory distress, umbilical cord discharge, hypertonia, tachycardia, bulging fontanelle and stiff neck between the two study sites. Missingness was uncommon and no adjustment or imputation was undertaken.
Neonates with PIH were referred to CURE Children’s Hospital of Uganda, a neurosurgical specialty hospital located in Mbale for further management. Additional specimens of CSF were collected as part of the neurosurgical evaluation. Each specimen was split into two aliquots: one that was collected into DNA/RNA preservative (DNA/RNA Shield, Zymo Corporation) and frozen at -80° C and one that was frozen without preservative. An additional 61 infants with PIH had their CSF processed in the same manner. The fresh frozen samples were thawed and 1 mL of CSF from each patient was inoculated into a BD BACTEC lytic anaerobic medium blood culture bottle supplemented with 1 mL of defibrinated horse blood (Thermo Scientific). Culture bottles were incubated in a BD BACTECTM FX instrument and monitored for bacterial growth for up to 14 days. Culture bottles that were positive for bacterial growth were subcultured on BD BBLTM Chocolate II and CDC Anaerobe 5% Sheep Blood agar plates and incubated at 37° C under anaerobic conditions (Anoxomat, Advanced Instruments). Culture bottles that remained negative after 14 days were also subcultured under anaerobic conditions though none of these resulted in bacterial growth. All subsequent culturing after initial anaerobic conditions was done aerobically. Three CSF samples were positive for growth in culture bottles. As previously described, colonies from subculture plates were used for Gram stain, organism identification by MALDI-TOF, biochemical testing, and antimicrobial susceptibility testing. Biochemical testing was performed using API 50 CH strip following manufacturers protocol. Susceptibility testing and interpretations were performed by E-test method using Clinical and Laboratory Standards Institute (CLSI) guidelines.
This study was approved by the Human Subjects Protection Program at The Pennsylvania State University, Pennsylvania, United States, by CURE Children’s Hospital of Uganda Institutional Review Board, the Mbarara University of Science and Technology Research Ethics Committee, and with oversight of the Ugandan National Council on Science and Technology. Informed written consent was obtained from each patient’s mother prior to enrollment. All data produced in the current study are available upon reasonable request to the authors and will be made publicly available once the parent neonatal sepsis study is published.
Results
Clinical Epidemiology of Paenibacillosis
Six percent (37/631) of neonates with clinical sepsis had PCR evidence of Paenibacillus infection. CSF PCR was positive in most cases, 35/631 (6%) patients; 1/35 (3%) of these also had a positive blood PCR. Two additional patients had a positive blood PCR but negative CSF PCR (Supplemental Table 1).
Paenibacillus genus and Paenibacillus thiaminolyticus qPCR results from blood and cerebrospinal fluid.
Demographics of neonates with clinical sepsis due with and without Paenibacillus thiaminolyticus detected by qPCR.
Postnatal age at presentation was similar for neonates with and without paenibacillosis, median age 3 (IQR 1, 7) days and 2 (1, 4) days, respectively, P=0.129 (Table 1). Most neonates with paenibacillosis were born vaginally (73%) in a healthcare facility (hospital, lower level health center or private clinic) (78%). However, when compared to infants without paenibacilliosis, infants with paenibacilliosis detected were significantly more likely to be born at home, 6% vs. 22%, respectively, P<0.01 and to have received non-recommended cord stump care, 19% vs. 38%, respectively, P=0.01.
Neonates with paenibacilliosis frequently had fever (92%) and irritability (84%) (Figure 1). Clinical seizures were present in half of neonates. A bulging fontanelle was present in 22% overall and in 6/16 (38%) infants at Mbale but in only 2/21 (10%) at Mbarara, P=0.06. All other presenting signs occurred in a similar proportion of neonates at each of the two sites.
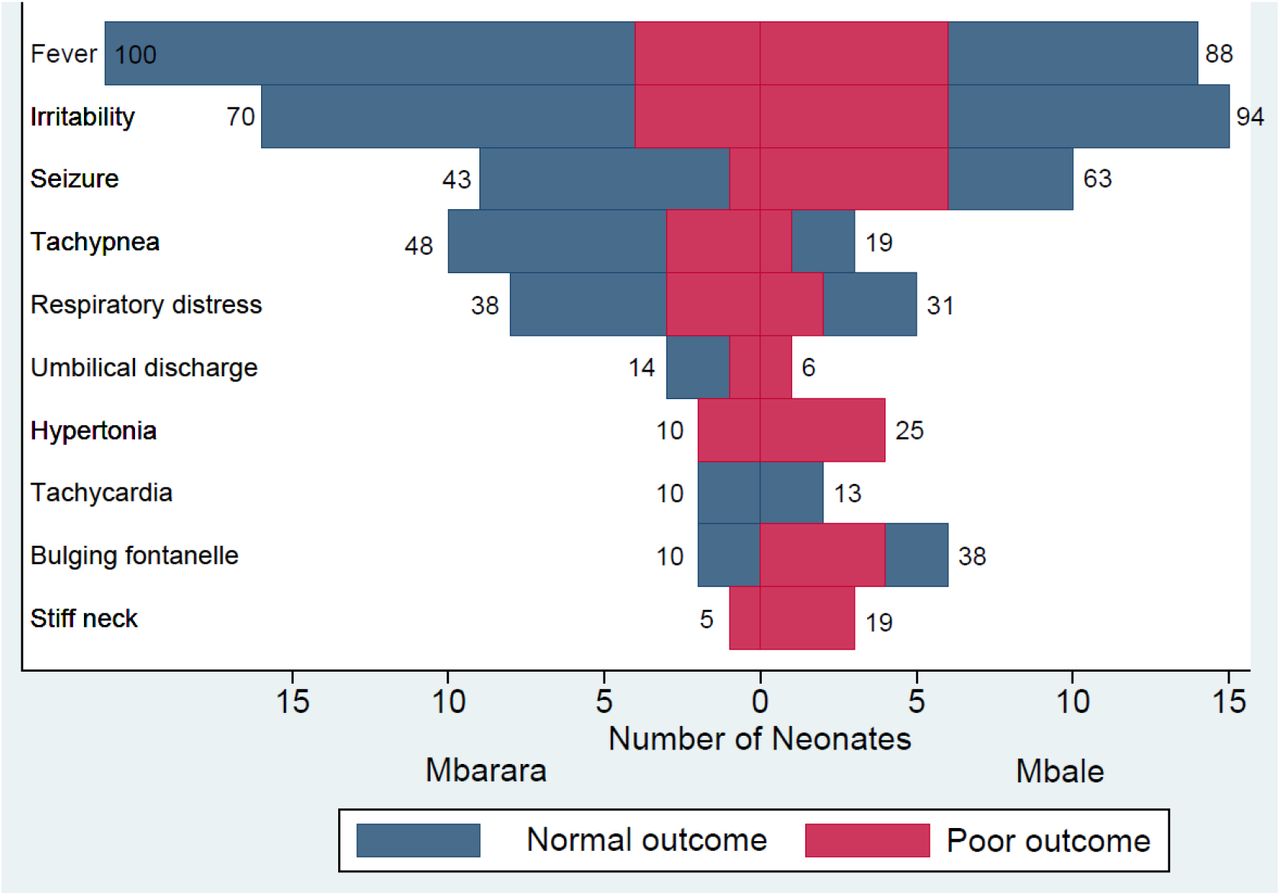
Presenting signs and outcomes for neonates with Paenibacillus thiaminolyticus detected by qPCR during clinical sepsis.
Number of neonates presenting to each site with each sign of infection. Numbers at the end of each bar indicate the proportion of neonates at each site who had the corresponding sign of infection. Neonates with the composite poor outcome of death, postinfectious hydrocephalus or moderate/severe neurodevelopmental impairment are indicated in red.
Laboratory studies
Blood cultures grew an organism in 4/37 (14%) of neonates (Supplemental Table 2). Two grew Staphylococcus aureus, and one each grew a Klebsiella species, a Bacillus species and Streptococcus agalactiae. Due to testing limitations at the local microbiology laboratory, species-level identification of some organisms was not performed. One of the neonates with S. aureus died shortly after hospital admission. All 37 neonates had negative antigen testing for malaria. Thirty-six patients had a blood CMV PCR performed; none was positive.
Results of blood polymerase chain reaction tests for cytomegalovirus and blood cultures for neonates with and without Paenibacillus detected.
Description of neonates who developed postinfectious hydrocephalus following neonatal sepsis with P. thiaminolyticus detected by qPCR
Seventeen of the 37 paenibacilliosis patients had a CSF WBC count reported. Four of the 17 (24%) neonates with an available CSF WBC count had a CSF WBC count ≥ 15: 20, 75, 75 and 80 ×106 cells/L. The protein concentration was ≥ 1 g/L in two of these four (50%) neonates (1.8, 5.4 g/L) and in an additional 6 neonates (8/37, 22%) with normal or unavailable CSF WBC counts (1, 1, 1, 2.3, 3.4, 5 g/L). CSF and blood glucose concentrations were not available. No CSF culture grew bacteria in the local laboratory.
Treatment
The choice of empirical therapy was chosen by the admitting healthcare worker and therefore varied across the cohort. Most neonates with paenibacilliosis (26/37, 70%) were initially started on intravenous ampicillin plus gentamicin. Eight (21%) were treated initially with a third-generation cephalosporin (ceftriaxone or cefotaxime) along with either gentamicin (5, 13%), or an aminoglycoside, ampicillin and cloxacillin (2, 7%). Three (8%) received ampicillin, cloxacillin and gentamicin as initial therapy and 1 (3%) received ampicillin, gentamicin and ceftriaxone.
Antibiotic therapy was escalated to a broader antibiotic regimen for 9/37 (24%) neonates. Antibiotic escalation occurred after a median of 3 days (IQR: 3, 3). This is common practice in these hospitals, when the treating clinician does not see a good clinical response. Most commonly, ampicillin was changed to a cephalosporin (5/9, 56%). In two cases each (2/9, 22%), cloxacillin was added to ampicillin and gentamicin and in 1 case (1/9, 11’%) gentamicin was changed to a cephalosporin and ampicillin was continued.
Outcomes
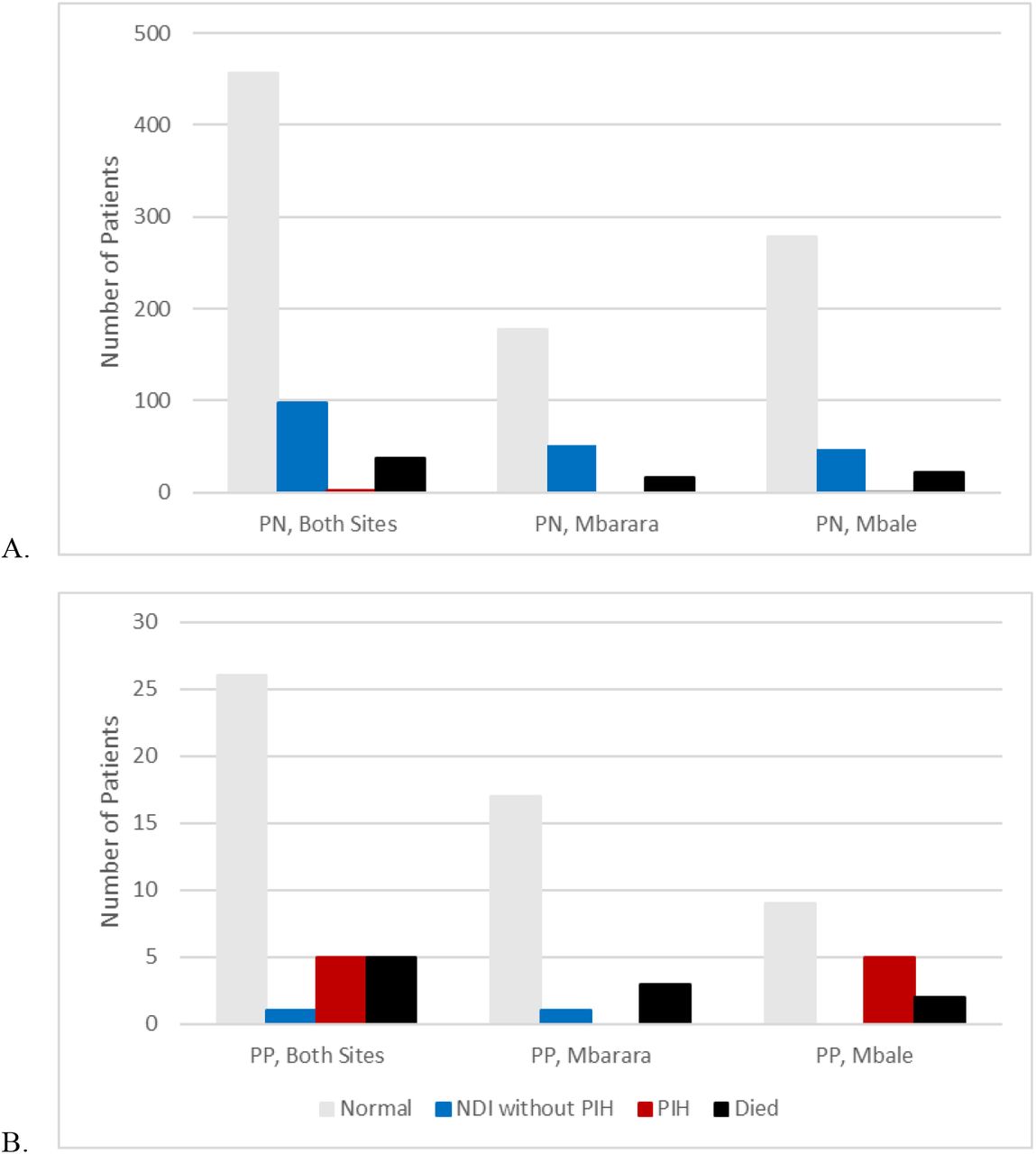
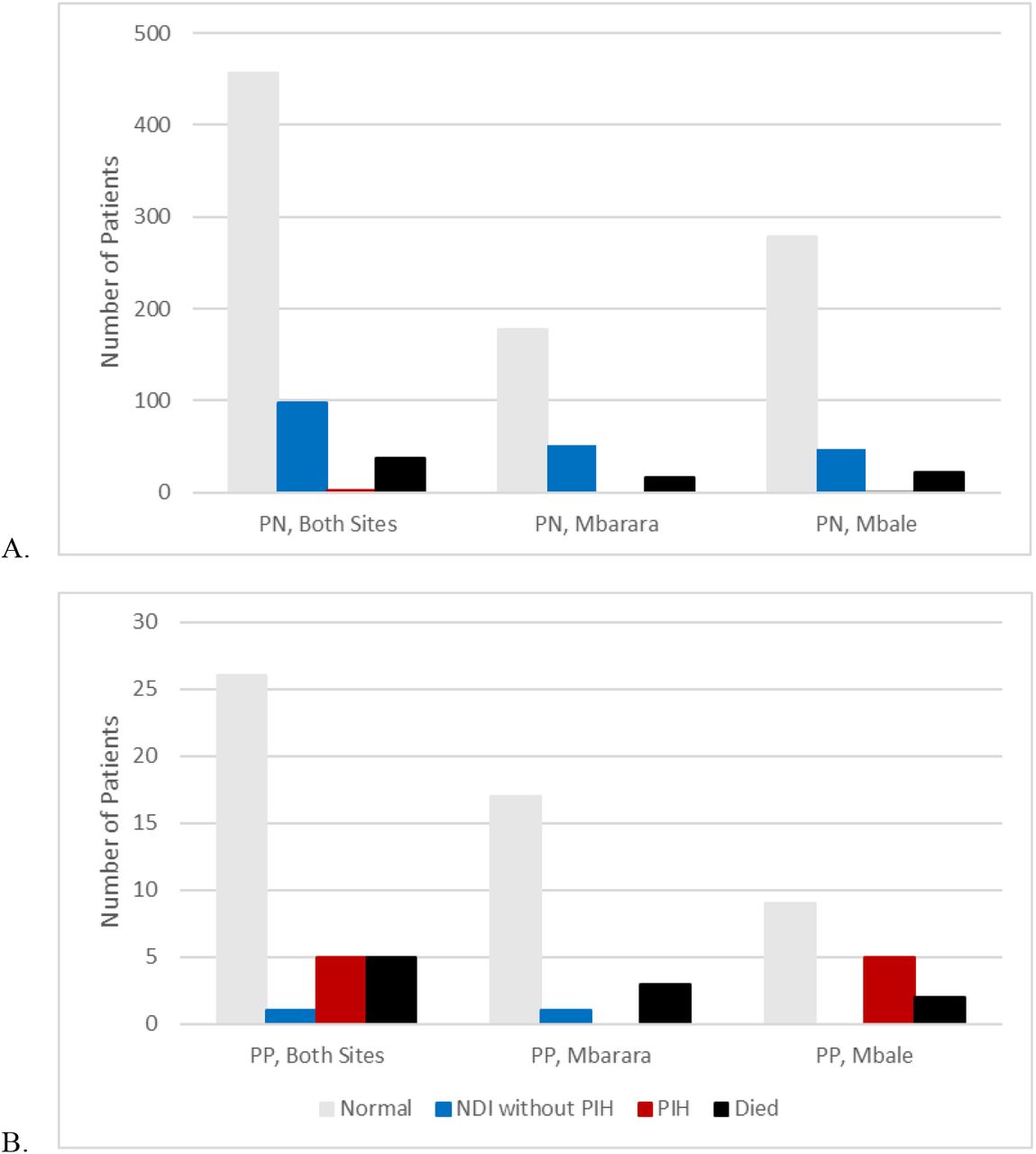
The composite poor outcome of infant death, PIH or NDI was more common in neonates with paenibacilliosis than those without, 11/37 (30%) vs. 79/594 (13%), P=0.012. Among neonates with paenibacilliosis, there was no difference in the frequency of the composite poor outcome between the two sites, 7/16 (44%) at Mbale and 4/21 (19%) at Mbarara, P=0.151 (Figure 2). Infant death following paenibacilliosis occurred in 5/37 (14%) and occurred in a similar proportion of neonates cared for at each site, 2/16 (13%) at Mbale and 3/21 (14%) at Mbarara, P=1.00. Three patients progressed rapidly to death prior to hospital discharge. Another infant remained critically ill during the hospital stay and was discharged to home against medical advice; this infant died shortly after discharge home. A fifth patient was treated with 5 days of ampicillin and gentamicin, was discharged home from the hospital in good condition but developed a second febrile illness and died at 2 months of age.
{kind=link}
{kind=link}
Outcomes for neonates with clinical sepsis with Paenibacillus negative (PN) and Paenibacillus positive (PP) qPCR results for Paenibacillus thiaminolyticus detection in the CSF at both sites and at Mbarara and Mbale.
PIH was also more common among neonates with paenibacilliosis than those neonates without paenibacilliosis, 5/37 (14%) vs. 3/594 (<1%), P<0.001. Additionally, PIH occurred following paenibacilliosis more frequently at Mbale, 5/16 (31%), than at Mbarara, 0/21 (0%), P=0.010. Four of the five (80%) neonates with Paenibacillus-associated PIH had an elevated CSF protein concentration but all 5/5 (100%) had a CSF WBC count < 100 ×106 cells/L at presentation (Table 2). Two required placement of a ventricular peritoneal shunt, two were managed conservatively without surgery and one was referred for neurosurgical evaluation but was lost to follow-up. Nineteen of the 32 (59%) paenibacilliosis survivors had a developmental assessment performed at 6 months and 22/32 (69%) at 12 months; 29 (91%) had a developmental assessment at 6 or 12 months of age. Three of the 4 patients with paenibacilliosis-associated PIH who remained in care had moderate/severe neurodevelopmental impairment as assessed at 6- or 12-months of age (Table 3). One additional neonate (4%) who survived without hydrocephalus had NDI at the last developmental assessment.
Developmental outcomes for survivors of neonatal sepsis with P. thiaminolyticus detected by qPCR
The three isolates of P. thiaminolyticus that were successfully cultured from infants with PIH following NS were all non-susceptible to vancomycin (Table 4). Two of the three (67%) were resistant to ampicillin. There are not interpretive criteria for the clinical significance of minimum inhibitory concentrations (MIC) for ceftriaxone but 2 of the 3 had a very low MIC and the third had an MIC of 0.25 ug/mL, a concentration which is probably susceptible.19
E-test Antibiotic susceptibility testing results for P. thiaminolyticus isolates obtained from 3 infants with post-infectious hydrocephalus as a sequela of neonatal sepsis.
Discussion
We describe the first cohort of neonates with sepsis due to Paenibacillus species; most infections were due to P. thiaminolyticus. Signs of meningitis such as irritability, seizures and bulging fontanelle were common at presentation. Eleven percent of neonates died during their original in-patient admission. Poor outcomes were common among survivors: PIH developed in 16% and NDI was common.
P. thiaminolyticus has rarely been reported as a cause of human disease. The first case of human infection was reported in 2008 when an 80-year-old man undergoing hemodialysis developed bacteremia due to P. thiaminolyticus.20 He received 4 weeks of vancomycin and improved. A 33-year-old Swiss woman experienced a surgical wound infection due to P. thiaminolyticus 7 days following an abdominoplasty procedure.21 The organism was identified on culture of an aspirate from an abdominal wall fluid collection. She was treated with 2 weeks of unspecified intravenous antibiotics followed by 2 weeks of amoxicillin-clavulanate as definitive therapy and completely recovered. Finally, P. thiaminolyticus was recovered on blood culture from a 25-day old neonate admitted to a hospital in the United States of America due to cardiorespiratory arrest following 1 day of poor feeding and increased sleep.22 Unfortunately, the neonate succumbed to her infection 4 days later. Post-mortem examination revealed a soft brain with several areas of infarction but without clear signs of meningitis. Our finding that 33 of 631 (5%) neonates evaluated for sepsis had P. thiaminolyticus detected using molecular methods was unexpected and suggests that P. thiaminolyticus may be an underdiagnosed cause of neonatal sepsis, meningitis, and PIH in Uganda.
Studies seeking to identify causative organisms for neonatal sepsis may fail to identify P. thiaminolyticus for several reasons. First, this organism may have ecological niches that are not universally distributed. We failed to find any evidence of P. thiaminolyticus presence in the vaginal microbiome of 99 women residing in Mbale or Mbarara, Uganda at the time of delivery suggesting that neonates may become colonized with the organism through environmental, rather than maternal sources.23 It has been identified in fish from Lake Michigan in the United States,24 and from the soil in India.25 Other species of Paenibacillus have been identified in the soil globally26-30 and as a member of the human gut microbiome.31 Some species are known to infect honeybees32 and, rarely, humans.33-35 Neonates cared for in industrialized or high-resource settings may have limited contact with environmental reservoirs of Paenibacillus. Studies evaluating neonatal pathogens in high-resource settings may fail to identify Paenibacillus because there are no neonatal infections in those cohorts caused by Paenibacillus.
Neonates who are born and live in environments where exposure to contaminated water and soil is common could encounter Paenibacillus more frequently and at higher levels. It is possible that neonatal infections due to Paenibacillus do occur globally but are not diagnosed in either high- or low-resource settings due to the limitations of culture-based pathogen detection methods in neonates. Even common neonatal pathogens can be missed when the blood volume used to inoculate the blood culture bottles is <1 mL.36,37 Low sample volume will similarly have limited our ability to detect Paenibacillus in an infant with paenibacillosis. Blood cultures are typically incubated for 5-7 days and CSF cultures for 2-5 days. Paenibacillus may take 7-14 days to reach the level of detection using standard culture methods.38 Cultures may be deemed negative and the specimens discarded prior to sufficient time to detect Paenibacillus elapsing. Studies attempting to diagnose the spectrum of pathogens causing disease in neonatal sepsis may be improved by increasing the duration of specimen incubation beyond the standard 5-7 days or by using molecular methods to improve diagnostic yield.
In our prior work, we were able to grow P. thiaminolyticus from the CSF of 3 neonates with PIH by inoculating the CSF into anaerobic lytic blood culture bottles. Anaerobic blood culture bottles are not used as routine part of the evaluation of neonatal sepsis in most clinical settings but have been shown to increase the diagnostic yield of blood cultures for neonates with bacteremia.39 Culture sensitivity for fastidious organisms such as Kingella kingae is also known to be improved when synovial fluid is incubated in a blood culture bottle.40,41 The addition of an anaerobic blood culture bottle to the CSF evaluation of neonates with sepsis may improve the diagnosis of infections due to Paenibacillus and facultative anaerobes implicated in neonatal sepsis. Using these methods in all neonates with sepsis may not be warranted if the prevalence of infections identified using them is low. However, in research settings that attempt to describe the range of organisms infecting young infants expanding culture-based techniques to include additional types of media could potentially reduce false negatives and allow for a more complete description of the causative bacterial agents.
All of the neonates in our cohort with paenibacillosis were diagnosed using molecular methods. The addition of a Paenibacillus PCR to the evaluation of neonatal sepsis could improve the diagnosis of this emerging infection by providing a rapid, low-biomass way of identifying affected neonates. PCR and other molecular methods have been shown to be useful for the diagnosis of other fastidious organisms that cause disease in neonates such as Mycoplasma hominis,42 Ureaplasma parvum,43 Leptotrichia amnionii,44 and Sneathia amnii.45 Epidemiological studies of neonatal serious bacterial infections that only use culture-based methods likely underestimate both the number and variety of infections caused by bacteria.
The diagnosis of Paenibacillus infection is important for the care of neonates with sepsis due to the high incidence of associated mortality and morbidity. In contrast to infections due Streptococcus agalactiae (0%46-4%47), paenibacillosis resulted in PIH in 12% of cases. Meningitis due to E. coli causes PIH in 1847-22%46. In our cohort, Paenibacillus conferred a similar risk of PIH as E. coli but was a more common cause of infection in our cohort (data not shown). Thus, paenibacillosis may be a leading cause of PIH in Uganda. It is unknown whether optimal treatment of neonatal paenibacillosis would reduce the incidence of PIH or NDI in the region. We assessed NDI using the BSID-III. Although the BSID-III uses age-based normative values generated from an American population, the tool has been shown to be a valid means of comparing development for young African infants to each other but not to infants from other regions of the world.48,49 We found that NDI occurred following clinical neonatal sepsis in a similar proportion of infants with and without paenibacilliosis.
The World Health Organization recommends using the combination of ampicillin and gentamicin as the empirical antibiotic regimen for neonatal sepsis due to the coverage provided against Streptococcus agalactiae (Group B streptococcus), Escherichia coli, and Listeria monocytogenes.50 Regions where antibiotic resistance is common or additional organisms are typical may need to use a broader spectrum regimen empirically.51,52 Our discovery that P. thiaminolyticus could be a common cause of culture-negative sepsis in Uganda has important implications for empiric antibiotic selection. Antibiotic susceptibility testing performed on the three isolates we successfully isolated from neonates with PIH demonstrated resistance to ampicillin and vancomycin. We additionally identified the presence of several beta-lactamase genes which could confer resistance to ampicillin.53 Prior studies have found that resistance to ampicillin, vancomycin, clindamycin and tetracycline is common in Paenibacillus species.21,54 Because there are few clinical reports of P. thiaminolyticus, it is unknown how often resistance occurs or what antibiotic regimens would maximize the likelihood of a good outcome.
Inappropriate empirical antibiotic therapy has been associated with worse outcomes for neonatal sepsis. 55-57 These studies assume that an appropriate antibiotic is ultimately administered within 1-3 days of symptom onset.58 Unfortunately, P. thiaminolyticus can be difficult to recover using culture and will be consistently missed in Uganda and other parts of the world where neonatal sepsis is common.59,60 Thus, it is likely that many infected neonates do not receive effective antimicrobial therapy at all, thus increasing the risk of mortality and serious sequelae, including PIH. Incorporating the possibility of a difficult-to-culture organism into antibiotic guidelines and protocols has the potential to improve outcomes. Our findings suggest that the combination of a third-generation cephalosporin and gentamicin would be preferred over ampicillin and gentamicin as an empiric antibiotic regimen for neonatal sepsis in Uganda especially when meningitis is suspected. A prior study of soil Paenibacillus species’ suggests that ∼70% of isolates are susceptible to ceftriaxone, an antibiotic that has good penetration into the central nervous system.54 Gentamicin is less reliable at achieving therapeutic concentrations in the central nervous system, especially if an abscess is present, but resistance appears to be quite uncommon.54,61 Antibiotic susceptibility testing should be performed to guide antibiotic management in individual cases of paenibacilliosis. Performing antibiotic susceptibility testing on a larger number of isolates will be important to improve our understanding of how best to care for neonates with these infections.
The possibility of antibiotic resistance should be considered when antibiotics are chosen to treat a neonate with paenibacilliosis.62 In particular, the WHO-recommended first-line antibiotic regimen for the treatment of neonatal sepsis (ampicillin plus gentamicin), is unlikely to be effective for P. thiaminolyticus. Vancomycin is commonly used for gram positive central nervous system (CNS) infections and is the drug-of-choice for CNS infections due to Bacillus species but should not be used empirically for treatment of Paenibacillus infections.63 It is possible that alternate antibiotic regimens may be optimal for treatment of this novel infection. Because this organism may be an important pathogen in the developing world, any antibiotic consideration would need to achieve therapeutic concentrations in the CNS, be inexpensive, easily administered, and well tolerated with few side effects.
Nutritional interventions may also be important adjunctive treatments for P. thiaminolyticus infections. This organism produces thiaminase, an uncommon bacterial enzyme which has the potential to reduce thiamine levels.24 Recent studies have failed to show a mortality benefit of the combination of thiamine, vitamin C with and without hydrocortisone in mortality outcomes for adults with sepsis.64-66 However, in a retrospective analysis, thiamine supplementation improved survival for adults with hospital-acquired pneumonia.67 Thiamine supplementation may yet have a role for certain types of infection, in cases when sepsis is caused by a thiamine-consuming organism or when pre-existing thiamine deficiency exists.68-70 Furthermore, thiamine supplementation may improve neurodevelopmental outcomes or reduce the likelihood of other sequelae, such as PIH, following neonatal sepsis even if it does not infer a survival benefit.71,72 Studies evaluating the role of thiamine supplementation as adjunctive therapy for neonatal sepsis due to thiaminase-producing P. thiaminolyticus are needed.
An important area of future research will be to define the qPCR level that is clinically significant. In this report, we included all neonates who had any Paenibacillus result. It is possible that some infants included had infections due to other organisms, or even non-infectious reasons for presenting with clinical signs consistent with infection. Additionally, the outcomes that we present following neonatal paenibacilliosis may reflect inadequate antibiotic therapy being more common among neonates with Paenibacillus detected than those without. Infants with paenibacilliosis may be more likely to receive ineffective antibiotic therapy than infants without paenibacilliosis. This could explain some of the increased frequency of poor outcomes in infants with Paenibacillus detected. Since the causative pathogen was unknown in the majority of non-paenibacilliosis cases, we were not able to assess antibiotic-microbe concordance in order to assess for this possibility.
Conclusion
Paenibacillus species was identified in 6% of neonates with signs of sepsis who presented to two Ugandan referral hospitals; most of these were P. thiaminolyticus. Improved diagnostics for neonatal sepsis are urgently needed in the region. Optimal antibiotic treatment for this infection is unknown but ampicillin and vancomycin will be ineffective in many cases. The role of thiamine supplementation as adjunctive therapy is unknown but rational to consider.
Acknowledgements
This study and the parent neonatal sepsis study were funded by the National Institutes of Health under 1DP1HD086071(S.J.S) and 1R01AI145057 (S.J.S). J.E.E. was supported by National Center for Advancing Translational Sciences grant #KL2 TR002015.
Footnotes
↵Δ Deceased
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos