
ABSTRACT
Background Rheumatoid arthritis (RA) is an autoimmune disease that usually causes synovial inflammation, cartilage and bone deformity, and is associated with the production of rheumatoid factor (RF) and anti-citrullinated protein antibody (1-3). The ocular, cardiovascular and other systemic complications of this disease are of significant concern (4-6). In particular, the eye is susceptible to inflammation or autoimmune disorders and shows ocular manifestations that may be early clinical symptoms of systemic vasculitis in some rheumatic disease cases (7-8). This study used optical coherence tomography angiography (OCTA) to evaluate retinal and conjunctival microvascular alterations in RA patients.
Methods Twelve patients (24 eyes) with a history of at least 5 years of rheumatoid arthritis (RA) were identified from their medical records and compared with 12 normal controls (24 eyes). The microvasculature of each eye was measured quantitatively using OCTA images. The images were manually segmented into representations of two physiologic layers: the superficial retinal layer (SRL) and the deep retinal layer (DRL). The microvascular (SMIR, DMIR), macrovascular (SMAR, DMAR) and total microvascular (STMI, DTMI) density were quantified and calculated in each layer. Simultaneously, macular retinal area was segmented into different regions based on the hemisphere segmentation (SR, SL, IL, and IR), early treatment of diabetic retinopathy study (ETDRS; R, S, L, and I) and central wheel division methods (C1-C6). Microvasculature measurements were used to compare microvascular densities between RA and normal controls and to explore the correlation between microvascular alteration and disease.
Results Compared with the control group, superficial and deep retinal layer microvascular density was decreased in the RA group. The STMI (p<0.0001), DTMI (p<0.0001), SMIR (p<0.0001), and DMIR (p<0.0001), were lower in RA than in controls, while the SMAR (p=0.207), and DMAR (p=0.828), density was statistically similar between groups. A significant difference was found in both superficial and deep layers in S (p<0.0001), SL (p<0.0001 and p<0.0004 respectively), SR (p<0.0001 and p=0.008 respectively), IL (p<0.0001) and C1 (p<0.0001 and p<0.004 respectively), C2 (p<0.0001 and p=0.0002 respectively), C4 (p=0.02 and p=0.007 respectively) regions, and additionally in the L (p<0.0001), I (p=0.004), C3 (p<0.0001) and C5 (p=0.002), regions in the superficial layer. Similarly, the temporal conjunctival vessel density was found to be lower in RA patients than in controls (t=2.030; P=0.048). In RA group, a statistically positive correlation was indicated between conjunctival microvascular and STMI densities (correlation coefficient 0.712, p=0.02).
Conclusion RA is complicated by several severe ocular symptoms and causes superficial and deep microvascular density alteration. This finding could precede diagnosis of the underlying RA and may be a useful factor in early diagnosis and the avoidance of long-term sequelae in systemic rheumatic diseases.
INTRODUCTION
Rheumatoid arthritis (RA) is a systemic autoimmune disorder that affects multiple organs and predominantly the synovial joints, ultimately causing irreversible joint damage (9-10). Population-based research shows that the prevalence of RA rises with age, is highest in middle-aged females, and rare in males (11-12). The incidence has been reported as ranging from 5 to 50 per 100000 adults (13-14). The extra-articular complications of RA are present in 10–20% of patients at any age and are more common in seropositive patients (15). The ocular complications such as Sjögren’s syndrome, episcleritis, and scleritis may further threaten ocular prognosis, exacerbate the course and even increase mortality (16-17). Although RA is predominant in females, the extra-articular complication of the disease occurs more frequently in males (18). In patients with RA, tissue damage on the ocular surface is autoimmune-mediated. Defects in innate immunity, cytokines, chemokines, and T helper cell subsets have all been linked to disease etiology in people with eye complications, such as dry eye. In addition, the most frequent ophthalmological lesion in RA is dry eye, affecting about one in four RA patients (19-20), which may develop into secondary Sjögren’s syndrome (21-22) and damage the structure and function of conjunctival epithelial cells by increasing inflammatory mediators and causing ocular surface microvascular alterations (23). Comparison between the macular vascular density of the RA group and the normal control group may therefore provide a feasible approach to distinguish healthy eyes from those with RA. To date, the pathogenesis of RA is unclear but is understood to be multifactorial with variations in gene expression and protein translation (24).
Surface and deep vessels can be detected with optical coherence tomography angiography, making it easier to observe aberrant vascular alterations in the retina. OCTA is more advantageous to observe and research the fundus changes of patients than fundus fluorescein angiography since it is noninvasive, has higher resolution, and takes less time.
METHODS
Research subjects
In this prospective study, 12 patients (24 eyes) with adult RA and 12 normal controls (24 eyes) were recruited at the First Affiliated Hospital of Nanchang University. The normal participants were healthy individuals with no autoimmune disorder or ophthalmological lesion. Detailed ocular examination was conducted in each subject by the same retinal specialist after noting RA disease duration.
Recruitment criteria
Patients meeting the following criteria after examination were enrolled in the study: (1) Female (2) Between ages of 25 and 60. (3) Diagnosed with rheumatoid arthritis based on the 1987 or the 2010 American College of Rheumatology (ACR) criteria or European League Against Rheumatism (EULAR) criteria.
Exclusion conditions
Patients meeting any of the following were not eligible to participate: (1) Those with inflammatory joint diseases other than RA, such as arthrolithiasis, reactive arthritis, psoriatic arthritis or Lyme disease. (2) Systemic autoimmune diseases, such as scleroderma, inflammatory myopathy or systemic lupus erythematosus. (3) Ocular diseases other than RA. (4) Ophthalmic surgery within 6 months. (5) Pregnant or lactating patients.
Ethical considerations
This study was carried out in compliance with the principles of the 1964 Declaration of Helsinki. The study was approved by the ethics committee of the First Affiliated Hospital of Nanchang University. Informed consent was signed from all subjects prior to participation.
Clinical examination
All patients underwent ophthalmic evaluation and clinical examination including monocular assessment of visual acuity, intraocular pressure, erythrocyte sedimentation rate, C-reactive protein, autoantibody testing, injury index, blood pressure, disease duration and OCTA. The general information of participants and the ocular clinical findings were summarized in Table 1.
Clinical and demographic characteristics of control group and RA group
The visual acuity test was performed by one optometrist based on a decimal progression chart while comparing the mean visual acuity of both RA patients and controls.
OCTA
For depth-specific visualization of blood flow in retinal microvasculature, the RTVue Avanti XR system was used to conduct OCTA imaging (Optovue, Fremont, CA). The scan rate was set at 70,000 A-scans per second, with an 840 nm central wavelength and a 45 nm bandwidth. The horizontal resolution was 22μm, and the axial resolution was 5mm. Five angiographs were performed for a total of 216 A-scans along the X-axis. Each scan centered on the posterior pole, located at 216 raster positions (along the Y-axis) and the acquisition duration was 3.9 seconds. At 270 frames per second, the 1080 B-scans (216 y-positions × 5 positions) were conducted. The 6×6 mm OCTA images were acquired using four volume scans of 2 vertical scans and 2 horizontal scans. Finally, calculating three-dimensional 6×6 mm en-face OCT angiograms for each eye (25).
A split-spectrum amplitude-decorrelation algorithm was used to segment the retinal images. The three-dimensional OCTA images were manually segmented into representations of two physiologic layers: the superficial retinal layer (SRL), which is between the interface and anterior boundary of the ganglion cell layer, and the deep retinal layer (DRL), which is located between the inner and outer boundaries of the inner and outer plexiform layers. The study focused on both of these physiologic layers, analyzing the microvascular (SMIR, DMIR), macrovascular (SMAR, DMAR) and total microvascular (STMI, DTMI) density, respectively (Figure 1 A-H).

(A–H) Optical coherence tomography angiography image of the macular region of the retina. (I–P) Partition methods of the retinal microvascular. STMI: superficial total microvascular; SMAR: superficial macrovascular; SMIR: superficial microvascular; DTMI: deep total microvascular; DMAR: deep macrovascular; DMIR: deep microvascular.
The macular retinal image area was manually segmented using different partition methods as follows (25) (Figure 1 I-P): The area was divided into four quadrants using the early treatment of diabetic retinopathy study (ETDRS) approach, right (R), left (L), superior (S) and inferior (I) (Figure 1 J, N). The hemisphere segmentation method involved dividing the image into four diagonal quadrants, superior right (SR), superior left (SL), inferior right (IR) and inferior left (IL) (Figure 1 K, O). The central wheel division method, disregarding the central foveal area with a diameter of 0.6mm, was used to define the image as a 0.6 to 2.5 mm-diameter circular region with a bandwidth of 0.95 mm, which was then divided into six rings (C1–C6), each with a bandwidth of 0.16mm (Figure 1 L, P).
In addition, the beam width was set to 22 μm, the axial resolution to 5 μm, and the light source center to 840 nm for the conjunctival OCTA images. Scanning was done at a rate of 70,000 times per second. The distance between the lens adapter and the participant’s corneal surface was set to 2 to 4 cm. ImageJ was used to export the images (National Institutes of Health, Bethesda, MD). Scanned areas were determined as 4mm along the circumference of the limbus conjunctivae’s edge and 5 consecutive rectangles (100 pixels, 850 m). A specified filter was used to generate binary images for analysis, highlighting the microvascular structure.
Statistical analysis
The primary objective was to evaluate the association between macular vascular density and disease in patients with RA. Statistical software (GraphPad Prism version 9.0, Statistica version 7.1, MedCalc program version 10, MedCalc Software, Mariakerke, Belgium; and StatSoft, Inc., Tulsa, OK) was used to analyze all clinical data. The data are presented as means and standard deviations. To compare the two groups, an independent sample t-test was utilized. The P values were two-sided, and P values less than 0.05 were considered evidence of statistical significance. The receiver operating characteristic (ROC) curve was utilized to analyze the superficial and deep macular vascular densities between the RA and the normal control groups.
RESULTS
Clinical and demographic characteristics of control and RA groups
In this study, the 12 patients with rheumatoid arthritis (RA) were identified from their medical records and compared with the control group (12 participants) based on the following patient characteristics: age, gender, ocular clinical findings and demographic characteristics. Mean patient age was 39.00±9.74 years in the RA group and 38.92±5.78 years in the normal control group; the mean intraocular pressure was 15.46±1.56 and 14.95±1.07, respectively. No statistically significant difference was found in age, intraocular pressure, blood pressure, antiphospholipid antibody and SDI between the two groups (P>0.05). The SLEDAI-2K activity score for normal subjects was 0, while it ranged from 1 to 8 (mean 3.67±2.31) in RA (p<0.001). Additionally, the patients with RA had a significantly lower average visual acuity (0.69±0.26) than the control group (0.88±0.10, P=0.03). The ESR was 15.92±8.33 in RA, significantly higher that than in the normal control group (3.83±1.27, P=<0.001). Similarly, the CRP level was significantly higher in the RA group (3.26±2.46) than in controls (1.30±0.79, P=0.02). The above clinical data suggest that ocular symptoms of RA may be sufficient in severe cases to threaten visual function significantly. The above participant data are shown in Table 1.
Superficial macular vascular density
In this study, superficial microvascular densities were measured in each group using OCTA (Figure 2A, B). Compared with the control group, the STMI (P<0.0001) and SMIR (P<0.0001) densities were significantly lower in the RA patients, while the SMAR (P=0.207) density was not significantly altered in RA (Figure 2C). Using the EDTRS method, the superficial macular vascular density was decreased in the RA group in areas S (P<0.0001), L (P<0.0001), and I (P=0.004) (Figure 2D). In addition, the hemisphere segmentation and central wheel division methods also showed lower densities at SR (P<0.0001), SL (P<0.0001), IL (P<0.0001), C1 (P<0.0001), C2 (P<0.0001), C3 (P<0.0001), C4 (P=0.02), and C5 (P=0.002) regions (Figure 2E, F). In regions not specified here the densities were statistically similar in the two groups.

(A) The retinal microvasculature density in superficial macular areas was measured using an OCTA scan. The density of superficial total microvessels (STMI), superficial macrovessels (SMAR) and superficial microvessels (SMIR) were measured in the control and RA groups. (B) Intergroup comparison of the microvascular macular density in the superficial layer based on EDTRS, hemispheric segmentation and central wheel division methods. The red areas in Figure 2B indicate areas with significant differences between the groups. (C–F) Comparison of retinal vessel density between RA and control groups in superficial retinal layers.
Deep macular vascular density
The same approach was used to compare densities in the deep layer between groups (Figure 3A, B). Similar to findings in the superficial layer, the DTMI (P<0.0001) and DMIR (P<0.0001) densities were significantly lower in the RA group than in controls while DMAR density was similar between groups (P=0.828) (Figure 3C). Using the EDTRS method, the superficial macular vascular density was decreased in the S region (P<0.0001) (Figure 3D). The hemisphere segmentation and central wheel division method also indicated lower density in RA in the following regions: SR (P=0.008), SL (P<0.0004), IL (P<0.0001), C1 (P<0.004), C2 (P=0.0002) and C4 (P=0.007) (Figure 3E, F). The measurement results of microvascular density in specific regions of the deep retinal showed a statistical difference between the RA and normal controls by using the different retinal partition methods.
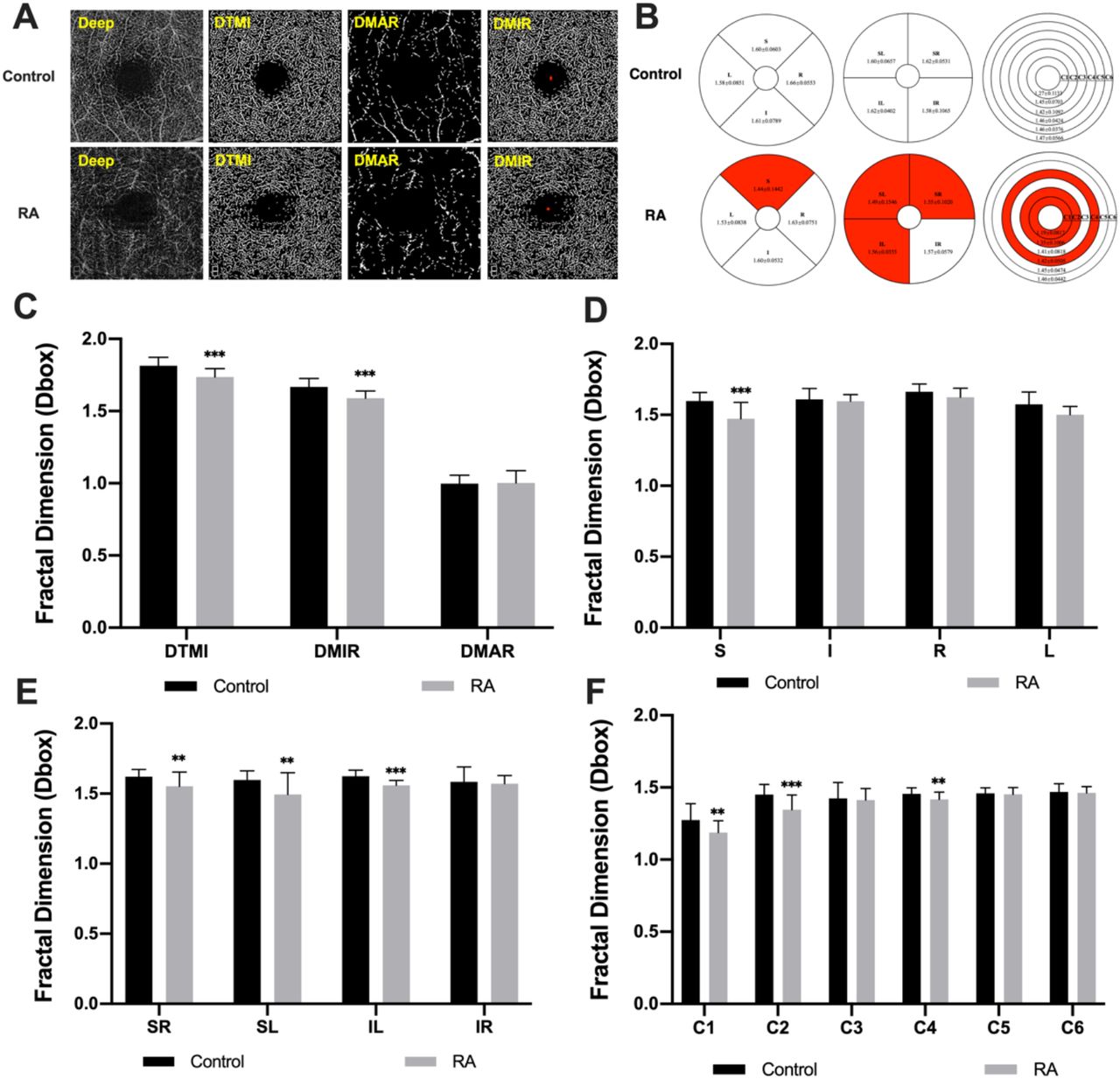
(A) The retinal microvascular density in deep macular areas was measured using an OCTA scan. The density of deep total microvessels (DTMI), deep macrovessels (DMAR) and deep microvessels (DMIR) was measured in the control and RA groups. (B) Intergroup comparison of the microvascular macular density in the deep layer based on EDTRS, hemispheric segmentation and central wheel division methods. The red areas in Figure 3B indicate areas with significant differences between the groups. (C– F) Comparison of retinal vessel density between RA and control groups in deep retinal layers.
ROC analysis of superficial and deep retinal vessel densities
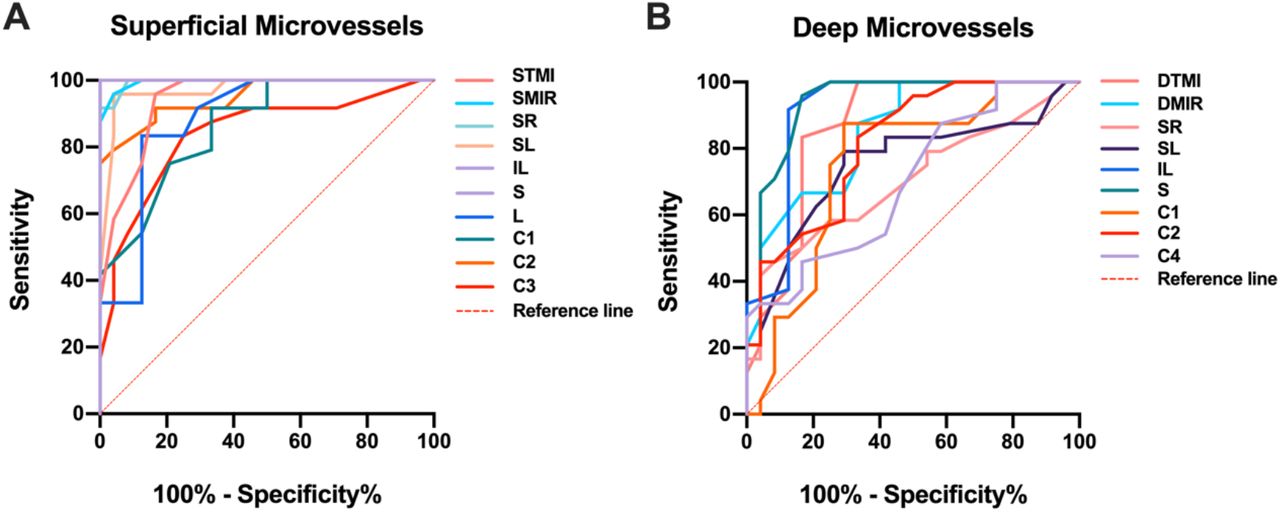
ROC curves provide an essential means of describing and comparing the accuracy of a diagnostic test in medicine. In the present study, superficial and deep retinal vessel density sensitivity and specificity were determined using each possible cut-off point on the curve and were found to be high (Figure 4). The IL and S regions showed the highest positive likelihood ratios and the area under the ROC curve was 1.00 (95% confidence interval [CI] = 1.00), while for density of the superficial retina of the I region, the lowest area under the ROC curve was 0.73 (95% confidence interval [CI] = 0.59–0.87) (Figure 4A). In the deep layer, the DTMI, DMIR, SR, SL, IL, S, C1, C2 and C4 regions were also significantly different between groups. The area under the ROC for the S region was 0.94 (95% confidence interval [CI] = 0.86–1.00) and showed the highest sensitivity in the diagnosis of RA, while the C4 region showed the lowest diagnostic sensitivity, with an area under the ROC curve of 0.70 (95% confidence interval [CI] = 0.55–0.85) (Figure 4B).

ROC curve analysis of microvascular densities in retinal regions, each curve showing comparison between RA and controls groups. (A) In the superficial layer, the area under the ROC curve was 0.942 (95% CI =0.878–1.000) for STMI, 0.995 for SMIR (95% CI = 0.983–1.000), 0.995 for SR (95% CI = 0.983–1.000), 0.971 for SL (95% CI = 0.928–1.000), 1.000 for IL (95% CI = 1.000–1.000), 1.000 for S (95% CI = 1.000–1.000), 0.884 for L (95% CI = 0.785–0.982), 0.863 for C1 (95% CI = 0.763–0.962), 0.949 for C2 (95% CI = 0.892–1.000) and 0.839 for C3 (95% CI = 0.723–0.956). (B) In the deep layer, the area under the ROC curve was 0.867 (95% CI =0.759–0.976) for DTMI, 0.850 for DMIR (95% CI = 0.744–0.956), 0.702 for SR (95% CI = 0.553–0.852), 0.750 for SL (95% CI = 0.607– 0.895), 0.914 for IL (95% CI = 0.824–1.000), 0.936 for S (95% CI = 0.863–1.000), 0.753 for C1 (95% CI = 0.607–0.898), 0.815 for C2 (95% CI = 0.697–0.934) and 0.700 for C4 (95% CI = 0.553–0.847).
Conjunctival vascular density
The temporal conjunctival vessel density was found to be lower in RA than in normal controls (t=2.030; P=0.048) (Figure 5A). Conjunctival vascular density and retinal superficial density in the STMI region were positively correlated (correlation coefficient 0.712, p=0.02) (Figure 5B).

(A) Comparisons of conjunctival vascular density between RA and control groups. (B) Relationship between retinal and conjunctival vessel densities.
DISCUSSION
The alterations in retinal capillary density in patients with RA were verified by OCTA. In both the superficial and deep macular regions of RA patients, the retinal capillary density reduced, especially in the superficial macular area, when compared to a healthy control group. Rheumatoid arthritis (RA) is a chronic systemic autoimmune disorder that affects multiple organs and predominantly the synovial joints (26). The prevalence range is reportedly from 5 to 50 per 100,000 adults and the peak incidence is in women aged 50 to 60 years. The pathogenesis of RA is known to be multifactorial but remains obscure (1,2727). The immunological pathogenesis is likely triggered by anti-citrullinated protein antibody forming immune complexes with citrulline-containing antigens and subsequently binding to rheumatoid factor further leading to excessive complement activation. The existence of these autoantibodies is related to severe joint damage and systematic symptoms (28). Patients with RA classically present with symmetrical pain and swelling of the synovial joints, causing recognizable longstanding joint deformities. However, some patients may present without typical joint symptoms, and in these patients recognition of RA may be delayed. The clinical course of RA is extremely variable, ranging from self-limiting joint symptoms to rapidly progressive multisystem inflammation with high mortality (29). Most notably, the innate and adaptive immune systems of the eye protect it against microbes and other immunological threats. Excessive immune system activation, however, causes inflammation and autoimmunity. In this study, we found that the aberrant eye manifestations play a critical role in the ocular complications of RA, which may represent local tissue ischemia and aberrant microcirculation. Among them, one of the locations affected is macular retinal capillaries. The EDTRS, hemispheric segmentation and central wheel division methods were employed in our study to evaluate retinal capillary density in superficial and deep macular areas while measuring conjunctival vessel density. Also, verifying that RA causes a decrease in retinal and conjunctival capillary density. However, the changes of retinal microvasculature in RA patients have no exact mechanism, but many studies have demonstrated that autoimmune diseases such as RA are often accompanied by ocular-related inflammatory complications (30-32). Thus, we infer that the long-term course of the disease may lead to the interaction between inflammatory cytokines and ocular capillary, further decreasing the overall microvasculature density and damaging the retinal capillary.
Therefore, the aim of the current study was to limit exacerbation of disease course by early RA diagnosis and prompt treatment. Delayed diagnosis may lead to chronic inflammation and irreparable joint or systemic organ damage. Ocular manifestations affect one quarter of RA patients (19-20). Whereas ocular indicators are often overlooked in disease assessment, existing research has shown that ocular symptoms are a marker of systemic disease activity.
Visualization and evaluation of the ocular microvasculature in RA patients are important for the treatment and prognosis of visual function, allowing for a more definitive diagnosis and assessment of disease activity during follow-up examinations. OCTA is a new technique, which can provide detailed microvascular morphology, information and greater quantification capabilities to achieve the objective of assessing the subtle changes for capillary beds in eye disease. (33-34). In addition, the ocular surface’s accessibility may provide a one-of-a-kind opportunity to investigate systemic pathogenic pathways without invasive testing. Once validated, ocular microvasculature might be used as biomarkers to monitor and possibly predict the progression of RA disease.
This is the first published study using OCTA to measure alterations in ocular microvasculature in patients with RA. This study found decreased retinal microvascular density compared to normal controls, consistent with ocular symptoms in RA patients. Using OCTA to achieve early detection of changes to retinal circulation can prevent severe eye disease and facilitate early treatment of the disease to avoid blindness and disability, thus improving the prognosis of RA patients. However, this study has several limitations based on the small sample size. A longitudinal cohort study with a large sample size should be conducted to objectively evaluate the retinal microvasculature changes in patients with RA. In addition, further research should be conducted on diagnostic criteria for RA to comprehensively analyze ocular vascular changes as potential biomarkers for clinical diagnosis in this disease.
CONCLUSION
Rheumatoid arthritis includes sight-threatening ocular complications such as Sjögren’s syndrome, scleritis, keratolysis and peripheral ulcerative kerati tis (35-36). These ocular conditions may be recurrent or chronic and often need long-term therapy coordinated with rheumatoid disease signs (37-38). In the present study, the results of clinical examination demonstrate that visual acuity is poorer in RA than in controls. Simultaneously, the ESR and CRP levels used to diagnose and monitor inflammatory processes such as inflammatory arthritis (39) showed an increasing trend in patients with RA, while the average intraocular pressure was similar in the two groups. The OCTA images showed decreased macular microvascular density in superficial and deep retinal layers and a positive correlation between STMI density and the changes in temporal conjunctival microvasculature.
As the ocular surface plays such a critical role in defense microorganisms and other threats, the eye is susceptible to inflammation or immunologic disorders and shows different ophthalmological manifestations that may be early symptoms in some rheumatic disease cases, ahead of systemic vasculitis (40). This study found ocular microvascular changes which may precede the diagnosis of the underlying RA (41-43). Further clinical research on ocular manifestations of RA may help to determine whether ocular changes of this kind may provide reliable diagnostic indicators and help to avoid long-term sequelae in systemic rheumatic diseases.
Data Availability
All data produced in the present study are available upon reasonable request to the authors All data produced in the present work are contained in the manuscript
Footnotes
Conflict of Interest Statement: This was not an industry supported study. The authors report no conflicts of interest in this work.
Funding Disclosure: Key Research Foundation of Jiangxi Province (No: 20203BBG73059, 20181BBG70004); Excellent Talents Development Project of jiangxi Province (20192BCBL23020); Natural Science Foundation of jiangxi Province(20181BAB205034); Grassroots Health Appropriate Technology “Spark Promotion Plan” Project of Jiangxi Province (No:20188003); Health Development Planning Commission Science Foundation of Jiangxi Province (No: 20201032); Health Development Planning Commission Science TCM Foundation of Jiangxi Province (No: 2018A060)
Ethical Statement: All research methods were conformed to the ethical requirements of the First Affiliated Hospital of Nanchang University and were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The method and purpose of the study were informed and consented to all subjects prior to participation.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}