
Abstract
Aim of the study This systemic review and meta-analysis aimed to analyze post-operative morbidity after liver resection, and also study various factors associated with mortality via metaregression analysis.
Material and Methods PubMed, Cochrane Library, Embase, google scholar, web of science with keywords like ‘liver resection”; “mortality”;” hepatectomy”. Weighted percentage post-operative morbidities were analyzed. Meta-analysis and meta-regression were done by the DerSimonian-Liard random effect model. Heterogeneity was assessed using the Higgins I2 test. Publication bias was assessed using a funnel plot. Funnel plot asymmetry was evaluated by Egger’s test. Morbidity was defined as any postoperative morbidity mentioned.
Results A total of 46 studies was included in the final analysis. Total 45771 patients underwent liver resections. 16111 patients experienced complications during the postoperative period. Weighted post-operative morbidity was 30.2% (95 % C.I. 24.8-35.7%). Heterogeneity was high with I2 99.46% and p-value <0.01. On univariate analysis, major liver resections were significantly associated with heterogeneity. (p=0.024). However, residual heterogeneity was still high with I2 98.62%, p<0.001. So, multifactor metaregression analysis major hepatectomy (p<0.001), Open hepatectomy (p=0.001), cirrhotic liver (p=0.002), age (p<0.001), blood loss (p<0.001), and colorectal metastasis (p<0.001) independently associated with postoperative morbidity. Residual heterogeneity was moderate I2= 39.9% and nonsignificant p=0.189.
Conclusion Liver resection is associated with high postoperative morbidity and various factors like major hepatectomy, Open hepatectomy, cirrhotic liver, blood loss, and colorectal metastasis were associated with morbidity and responsible for heterogeneity across the studies.
Background
Liver resection is now established curative treatment for various malignant and benign liver pathology. Currently, Hepatocellular carcinoma and colorectal liver metastasis are the most common indications for liver surgery as well as primary and secondary liver malignancies. [1,2].
Perioperative care and surgical techniques for liver resections have improved significantly in the past few years, resulting in improved perioperative outcomes. Despite improved outcomes liver resection is still associated with very high morbidity and mortality. Also, there is a lack of uniformity in reporting the outcomes across various centers. [3,4,5]. Indications also vary with Europe having a predominance of colorectal cancer metastasis as indications whereas in Asia hepatocellular carcinoma is the most common indication for liver resection. [6].
This systemic review and meta-analysis aimed to analyze any post-operative morbidity after liver resection, and study various factors associated with mortality via univariate and multivariate metaregression.
Material and Methods
The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (2020) and MOOSE guidelines. [7,8]. We registered our protocol in the PROSPERO database [246263]. We conducted a literature search as described by Gossen et al. [9]. PubMed, Cochrane Library, Embase, google scholar, web of science with keywords like ‘liver resection”; “morbidity”;” hepatectomy”. Two independent authors extracted the data (B.V and H.P). We evaluated the last studies published in the last 5 years to see recent trends in 90 days mortality. In case of disagreements, decisions are reached on basis of discussions.
Definitions
We defined morbidity as any postoperative complications according to Clavien-Dindo classifications grade 1-5. [10]
Statistical Analysis
The meta-analysis was done using Review Manager 5.4 and the JASP Team (2020). JASP (Version 0.14.1)(University of Amsterdam). Weighted percentage morbidities with 95% confidence intervals were used. Univariate metaregression was done by DerSimonian-Laird methods. Major hepatectomy, Age, open surgery, cirrhotic livers, blood loss, hepatectomy for hepatocellular carcinoma, hepatectomy for colorectal liver metastasis were taken as covariates in metaregression analysis to study their association heterogeneity of the meta-\analysis. Factors with a p-value less than 0.05 were entered in the multivariate metaregression model and then we decided to check for residual heterogeneity, if residual heterogeneity is still significant, we decided to enter all co-variants in the multivariate model to look for mixed effects. Heterogeneity was assessed using the Higgins I2 test, with values of 25%, 50%, and 75% indicating low, moderate, and high degrees of heterogeneity, respectively, and assessed p-value for the significance of heterogeneity and tau2 and H2 value [11]. The random-effects model was used in meta-analysis. The random-effects model was used in meta-analysis.
Assessment of Bias
Cohort studies were assessed for bias using the Newcastle-Ottawa Scale to assess for the risk of bias [12,13] Publication bias was assessed using a funnel plot. Funnel plot asymmetry was evaluated by Egger’s test.
Inclusion and Exclusion criteria for studies
Inclusion criteria
Studies with full texts
Studies published in last 5 years.
Studies mentioning post-operative morbidity rates.
Studies which evaluated liver resections for different etiologies.
English language studies.
Exclusion criteria
Studies which were not fulfilling the above criteria.
Duplicate studies.
Studies which included analysis of liver resection for single etiology.
Results
Data extraction, study characteristics, and quality assessment
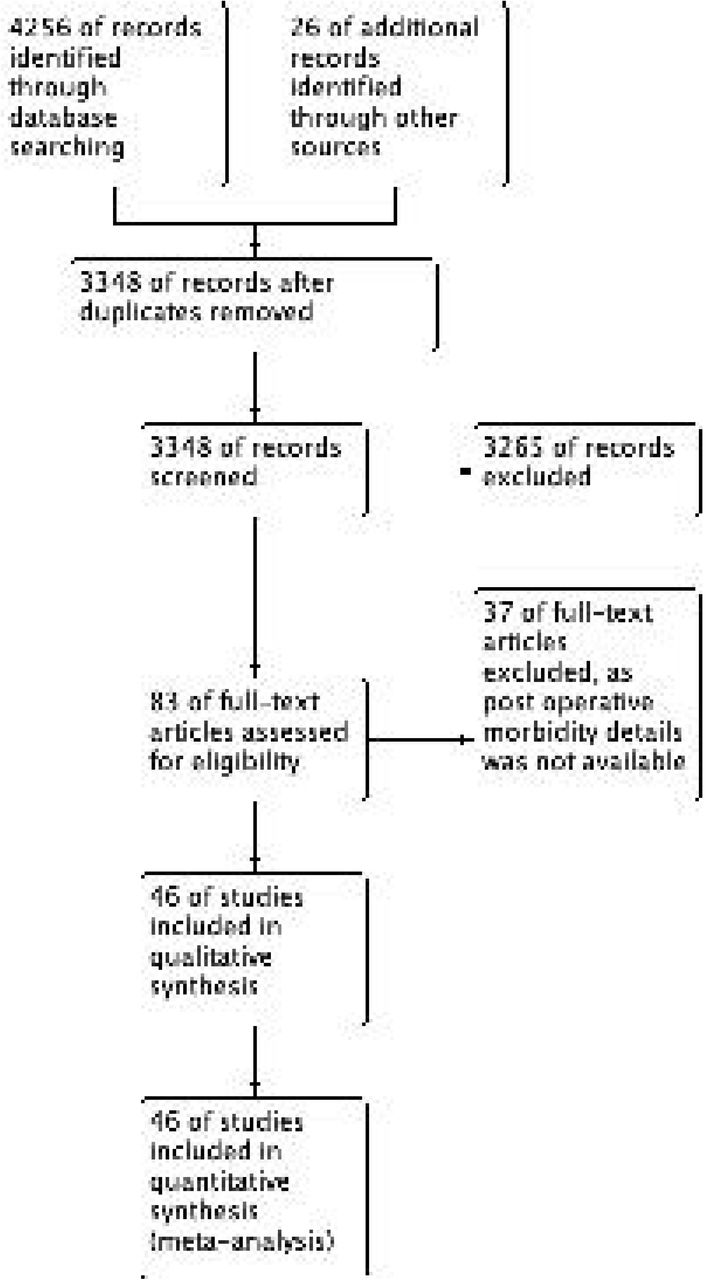
‘PUBMED’, ‘SCOPUS’, and ‘EMBASE’ databases were searched using keywords and the search strategy described above. Initially, 4256 studies published in the last 5 years were screened from the above search strategy, and 26 additional records were screened from references of the above studies. After removing duplicates 3348 studies screened again. 3265 studies excluded meeting the exclusion criteria. 83 full-text articles were evaluated. 37 full texts article removed as they did not mention post-operative morbidity rates.46 studies were included in the final qualitative and quantitative analysis. The risk of bias summary is mentioned in Figure 2. Study characteristics are mentioned in table 1. All except one study included are either retrospective studies or propensity score-matched analysis from retrospective data. In propensity score-matched analysis unmatched total data were analyzed for postoperative morbidity. Only one study was randomized control trial[51] in that also we analyzed total complications in both the group and total population. So, effectively all the data were retrospective.
Study characteristics.

PRISMA flow diagram.

Risk of Bias Summary.
Weighted post-operative morbidity
A total of 46 studies was included in the final analysis. [14-58]. Total 45771 patients underwent liver resections. 16111 patients experienced complications during the postoperative period. Weighted post-operative morbidity was 30.2% (95 % C.I. 24.8-35.7%). [Figure 3]. However, the heterogeneity of the analysis was high with I2 99.463%, tau2 0.034, and Q value of 8379.71, df 45. A p-value of heterogeneity was highly significant (p<0.001).

Forest plot of post-operative morbidity.
Publication Bias
Figure 4 mentions the funnel plot for publication bias. Egger’s test showed nonsignificant publication bias with a p-value of 0.202.

Publication bias for post-operative morbidity.
Metaregression analysis
We analyzed various covariates like major hepatectomy, Age of the patient, blood loss, open surgery, liver resections were done for hepatocellular carcinoma or colorectal liver metastasis and cirrhotic liver to check for their association with heterogeneity in the analysis and hence postoperative morbidity. On univariate analysis, only major hepatectomy was significantly associated with heterogeneity with a p-value of 0.024. However, residual heterogeneity was still highly significant with I2 is 98.5%, Q value 2988.013, df 41, Tau2 value of 0.015. So, we entered all the factors in the multiple meta-regression model.
Multiple metaregression model
On multiple metaregression model major hepatectomy (p<0.001), open surgery(p=0.001), cirrhotic background (p=0.002), age (p<0.001), blood loss (p<0.001) and liver resection for colorectal liver metastasis (p <0.001) were significantly associated with residual heterogeneity and hence postoperative morbidity. [Table 2]. Heterogeneity was significantly reduced with residual heterogeneity was non-significant with I2 of 39.99%, Q value 3.33, df 2, with the nonsignificant p-value. (p=0.189). Forest plot of multiple metaregression is included. [Figure 5]. Publication bias was nonsignificant with p=0.299. [Figure 6]. Diagnostic plots after multiple meta-regression analyses are shown in Supplement Figure 1.
Multiple meta-regression of various factors.

Forest plot of multiple meta-regression. (Observed outcomes fitted vs standardized outcomes calculated)

Funnel plot for studies mentioning all the factors in multiple metaregression.
Discussion
Liver resection is a curative surgery for many benign and malignant disorders, with the most common indications are hepatocellular carcinoma and colorectal liver metastasis. Liver resection was historically associated with very high morbidity and mortality, which has now decreased significantly due to improved surgical and anaesthetic techniques and improved perioperative and critical care. Complications and hence morbidity rates though decreased but remain very high and range between 20-40%. [14-58]. There are also wide regional variations in indications of liver resections. In Asian countries, the most common indication is hepatocellular carcinoma [59] while in European countries most common indication is colorectal metastasis, which can also be the reason for variable mortality following liver resection.
Our aim in conducting this systemic review and prevalence meta-analysis to study weighted post-operative morbidity rates after liver resections. We also aimed to look at the heterogeneity of the analysis and publication bias. We also did metaregression analysis for various factors affecting mortality like Major hepatectomy, blood loss, age, open resections, a cirrhotic background of the liver, and etiologies for resections like hepatocellular carcinoma and colorectal metastasis in a study published in the last 5 year to look for recent trends.
As shown in figure 3, Weighted post-operative morbidity was 30.2% (95 % C.I. 24.8-\35.7%). However, the heterogeneity of the analysis was significantly high. On univariate metaregression, only major hepatectomy was significantly associated with heterogeneity and hence morbidity but residual heterogeneity was still significantly high. After multiple factor metaregression entering all above factors as covariates, residual heterogeneity was moderate and not significant with p=0.189 and I2 39.99%. Elimination of residual heterogeneity after metaregression suggested that the above factors were mainly responsible for variable outcomes across the centers.
On multiple factor metaregression major hepatectomy, age, open surgery, cirrhotic background, blood loss, and colorectal liver metastasis were associated with heterogeneity and morbidity. As shown in table 2 major hepatectomy, open surgery, and cirrhotic background were having positive metaregression coefficients and z value suggesting a positive relationship which means higher the number of major hepatectomies, open surgery and surgery on cirrhotic liver higher the chance of positive effect size and hence higher morbidities. Colorectal liver metastasis was having a negative metaregression coefficient and z value suggesting higher the number of liver resections for colorectal liver metastasis lower the effect size and hence morbidity.
Blood loss and age were having negative metaregression coefficients and z value suggestive of negative correlation or inverse relationship between effect size or morbidity and them. This might be due to patients with older age or more blood loss have higher post-operative mortality even before complications happen. Their positive correlation with 90 days postoperative mortality has been reported by us in a similar meta-analysis with metaregression analysis under review for publication and available as preprint online. [60]. Limitations of the meta-analysis were a large number of studies had to be excluded due to lack of complication data [61]. Also, we could not take into account center volume and surgeon’s experience. Another limitation was only 10 studies mentioned all the moderators however, the number of studies was adequate to conduct metaregression analysis.
However, to our knowledge, this is the first meta-analysis that evaluated weighted post-\operative morbidity rates and evaluated various factors responsible for heterogeneity and lack of significant residual heterogeneity after metaregression proved their effects on variable morbidity rates across the centers.
In conclusion, postoperative morbidity rates may vary according to centers based on various factors mentioned above. Major hepatectomy. In open surgery, the cirrhotic background may be associated with higher morbidities and liver resection colorectal liver metastasis may be associated with lower postoperative morbidity compared with other etiologies like hepatocellular carcinoma.
Figure Legends

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnostic plots after multiple metaregression.
Footnotes
Conflict of Interests: None
Funding disclosure: nothing to disclose.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos