
Abstract
Background Education is inversely associated with cardiovascular disease. Several mediators for this association have been established but a significant proportion of the protective effect remains unaccounted for. Mental health is a proposed mediator, but current evidence is mixed and subject to bias from confounding factors and reverse causation. Mendelian randomisation (MR) is an instrumental variable technique that uses genetic proxies for exposures and mediators to reduce such bias.
Methods and Results We used logistic regression and two-step MR analyses to investigate whether educational attainment affects risk of mental health disorders. We then performed observational and MR mediation analyses to explore whether mental health disorders mediate the association between educational attainment and risk of cardiovascular disease. Higher levels of educational attainment were associated with reduced depression, anxiety and cardiovascular disease in observational analyses [Odds Ratio (95% Confidence interval) 0.79 (0.77-0.81), 0.76 (0.73-0.79) and 0.79 (0.78-0.81) respectively], and MR analyses provided support for these reflecting causal effects [OR (95% CI) 0.72 (0.67-0.77), 0.50 (0.42-0.59) and 0.62 (0.58-0.66) respectively]. Both anxiety and depression were associated with cardiovascular disease in observational analyses [OR (95% CI) 1.63 (1.49-1.79) and OR (95% CI) 1.70 (1.59-1.82) respectively] but only depression was associated in the MR analyses [OR (95% CI) 1.09 (1.03-1.15)]. Roughly 6% of the total protective effect of education on cardiovascular disease was mediated by depression.
Conclusions Higher levels of educational attainment protect against mental health disorders and reduced depression accounts for a small proportion of the total protective effect of education on cardiovascular disease.
Introduction
Cardiovascular disease is a leading cause of global morbidity and mortality1. The association between socio-economic inequality and cardiovascular disease is well-established, with those living in deprived areas typically having much higher cardio-vascular mortality than those in the less deprived areas2. More specifically, disparities in educational attainment have recently been shown to affect cardiovascular disease using both conventional and genetic epidemiological techniques3 In the latter, cardiovascular risk was estimated to decrease by a third for every 3.6 years of additional full-time education past the age of eleven 4.
A number of well-recognised cardiovascular risk factors appear to act as mediators for education5. For example, low educational attainment is associated with increased tobacco smoking, higher BMI, and higher blood pressure which in turn are linked to increased risk of cardiovascular disease6. However, even taking these mediators into account, there is a significant proportion of the association between education and cardiovascular disease that remains unaccounted for.
Existing evidence suggests an association between mental health and cardiovascular disease as well as an association between education and mental health7,8. Consequently, mental health may be another potential mediator between education and cardiovascular disease. For example, educational inequality may lead to disparities in psychological development by affecting exposure to stressors, resources to cope with stress, and negative external societal perception9. Poor mental health could, in turn, lead to increased cardiovascular disease risk with proposed mechanisms including chronic inflammation10, increased sympathetic nervous system activation11, and increased cortisol exposure12.
Conventional observational studies help identify and quantify any associations between the two that may be due to causal effects. Those that have explored education, mental health and cardiovascular disease have, so far, proved inconclusive13,14. Furthermore, observational evidence can be subject to bias from confounding and reverse causation, and specifically in the context of mediation studies, to measurement error and collider bias15.
Mendelian randomisation (MR) is an instrumental variable technique that uses genetic variants as a proxy for an exposure of interest16. These variants are randomised at conception and therefore largely inherited independently from other variants affecting confounding factors. These variants are also unchanged throughout the lifetime and so are unlikely to be affected by outcomes of interest, therefore reducing bias from reverse causation. Thus, MR reduces the sources of bias that limit causal inference in conventional observational research and is an effective, complimentary tool in investigating potential causality.
Here, we specifically used two-step MR using summary data for each step. Two-step MR measures the exposure-mediator, exposure-outcome and mediator-out-come effects separately and is particularly useful when binary mediators are being measured individually. We utilised separate samples for the instrument and outcome summary data, thus providing greater sample sizes in some cases.
In this study, we used a complimentary approach utilising both observational and MR techniques to explore the relationship between education, mental health and cardiovascular disease. Elucidation of this causal pathway could have important implications for policymakers interested in both physical and mental health improvement.
Methods
Data availability: The data used for the observational analyses conducted in this study is available to qualified researchers upon application to the UK biobank (https://www.ukbiobank.ac.uk/researchers/). The data used for the MR analyses conducted in this study is publicly available via the cited references.
I. Observational analyses
Sample
Our observational analyses used data from the UK Biobank, a national health resource which recruited participants aged 39-72 years from 22 centres across the UK between 2006-2010. Details of recruitment are publicly available17. We excluded 814 individuals on the basis of consent withdrawal, reported aneuploidy, or mismatch between reported and chromosomal sex. We then applied the Medical Research Council Integrative Epidemiology Unit quality control procedure in order to restrict the sample to those of European ancestry18. The final sample size with complete phenotype measures was 333,525 with a mean age of 56.9 years (standard deviation [SD] = 8) and 54% females.
Measures
Educational attainment: Participants in the UK Biobank reported the levels of qualifications attained and the highest level of qualification was converted into number of years in education using the International Standard Classification for Education coding of educational attainment (See Supplementary Table S1). Mean educational attainment was 13.9 years (SD = 5.1).
Mental health problems: Individuals were classified as having had a mental health problem if they reported “Yes” to either of the routine survey questions “Have you ever seen a general practitioner (GP) for nerves, anxiety, tension or depression?” or “Have you ever seen a psychiatrist for nerves, anxiety, tension or depression?”.
Depression: Individuals were classified as having major depressive disorder if their hospital episode statistics and/or general practice linked health record showed a diagnosis of a depressive episode or recurrent episodes according to the International Classification of Disease (ICD) codes F32 and F33.
Anxiety: Individuals were classified as having anxiety disorder if their health record showed such a diagnosis according to ICD code F41.
The prevalence of these mediators in our sample was 34% for mental health problems, 2.9% for depression, and 1.4% for anxiety.
Cardiovascular disease: Individuals were classified as having cardiovascular disease if their health records showed at least one diagnosis of angina or myocardial infarction prior to recruitment classified by ICD codes I20 and I21 respectively. The prevalence of cardiovascular disease in the sample at the time of recruitment was 6%.
Additional covariates included age, sex, smoking status, hypertension, obesity, and socio-economic position. The methods for their classification and the respective prevalence figures are reported in the supplementary material (see Supplementary Information and Supplementary Table S2).
II. MR analyses
Genetic instruments
Educational attainment: 1271 independent genome-wide significant loci (p<5×10-8) were identified in a GWAS meta-analysis of educational attainment by Lee and colleagues (N = 1,131,881)19. Educational attainment was measured as years in education. The GWAS meta-analysed 71 cohorts of European ancestry measuring educational attainment. The median effect size of each allele of these lead variants was 1.7 weeks of schooling.
Mental health problems: 14 independent genome-wide significant loci were identified in a recent GWAS of a phenotype described as “broad depression” in UK Biobank data (113,769 cases and 208,811)20. Here, we report this phenotype as “Having had a mental health problem” instead. Individuals were classified as having had a mental health problem if they reported “Yes” to either of the routine survey questions “Have you ever seen a general practitioner (GP) for nerves, anxiety, tension or depression?” or “Have you ever seen a psychiatrist for nerves, anxiety, tension or depression?”. Cases with diagnosed bipolar disorder or schizophrenia or who were taking anti-psychotic medications were excluded. A number of participants were also excluded by inter-relatedness filtering.
Depression: 44 genome-wide significant loci were identified in a GWAS meta-analysis of major depressive disorder (135,458 cases and 344,901 controls) by Wray and colleagues21. A total of 29 samples containing individuals of European ancestry were included in the analysis. Major depressive disorder was defined by meeting DSM-IV or IC9-9/10 criteria either by clinician review of medical records or by expert interview.
Anxiety: A recent GWAS of anxiety disorder (7016 cases and 14,745 controls) identified one independent genome-wide significant locus22. Anxiety cases were recruited from seven different cohorts of European ancestry participating in the Anxiety NeuroGenetics Study with cases confirmed according to DSM-IV criteria. In order to improve instrument power, we relaxed the significance threshold to p<5×10-5 and identified 108 independent significant loci following LD clumping (r2<0.001, distance>10000 kb).
Cardiovascular disease: We used summary data from a recent GWAS meta-analysis from the CardioGRAMplusC4D consortium23. This included 48 cohorts with a total of 60,801 cases and 123,504 controls. The cohort studies typically defined a case as having a diagnosis of myocardial infarction or angina with several also requiring confirmation from angiographic evidence.
III. Statistical analysis
All analyses were performed using R (Version 3.6.2)24. A directed acyclic graph for the proposed causal relationships investigated is shown in Figure 1.

A diagram illustrating the proposed causal relationships between education, mental health and cardiovascular disease. Z1 and Z2 represent genetic proxies and U represents confounding factors.
Observational analysis: First, we used logistic regression to investigate the association of educational attainment with cardiovascular disease and with each of our mediators having adjusted for the effects of age and sex. Second, we analysed the effect of each of our mediators on cardiovascular disease and, in order to effectively isolate the mediator effects, adjusted for age, sex, educational attainment, smoking status, socio-economic position, hypertension, and obesity. When specifically analysing the effects of depression on cardiovascular disease, we additionally adjusted for the effects of anxiety and vice versa.
The proportion mediated statistic was calculated using the product of coefficients method as detailed in previous work25. The effect sizes were calculated using absolute risk differences as estimated from the odds ratios from our regression analysis and the known prevalence figures in UK Biobank. Standard errors were calculated using the delta method.
MR univariable analysis: The univariable analysis consisted of using two-sample MR methods applied in the TwoSample MR package 0.4.1826. We first ran our analysis using educational attainment as an exposure and each of our proposed mediators and cardiovascular disease as outcomes. We then repeated the analysis using each mediator as an exposure and cardiovascular disease as an outcome.
For these analyses, we used an inverse-variance weighted (IVW) approach in the main analysis 27, with additional statistical sensitivity analyses: weighted mode28, weighted median29, and MR Egger30. Each sensitivity analysis makes different assumptions about pleiotropy.
When using the anxiety disorder instrument, we performed MR Robust Associated Profile Score (MR RAPS) instead of IVW to improve estimation whilst using a relaxed p-value threshold for the instrument31. MR RAPS offers a greater robustness to pleiotropy when using many weak instruments, as we do here.
Two-step MR analysis: We next performed two-step MR using the TwoSample MR package 0.4.18. We used the results of our univariable MR analysis for the exposure-mediator step. For the mediator-outcome step we then used the residual multivariable MR method to calculate the effect of each mediator on cardiovascular disease having adjusted for the effects of educational attainment32. The estimates for each step were multiplied together to produce an indirect effect estimate and the proportion mediated statistic was then calculated as for the observational analysis (detailed above).
IV. Sensitivity analyses
The methods for our sensitivity analyses are presented in the supplementary material (see Supplementary Information). These analyses included MR Egger, Cochran’s Q Tests of Heterogeneity, mean of F (mF) statistics, MR Steiger, and bidirectional observational models. They also included an observational analysis of mental health and cardiovascular disease conducted without adjustment for other co-variates except for age and sex.
V. Exploratory analysis
In order to illustrate an approach for investigating multiple mediators between mental health and cardiovascular disease, we performed an exploratory analysis of a likely candidate based on existing evidence. This analysis investigates the role of tobacco smoking as a mediator between depression and cardiovascular disease. The methods are in Supplementary Material.
Ethical Considerations: UK Biobank has received ethics approval from the UK National Health Service’s National Research Ethics Service (ref 11/NW/0382).
Results
Association of education with cardiovascular disease
We found strong evidence to suggest that educational attainment has an inverse association with cardiovascular disease (see Figure 2). In our observational analysis, for every standard deviation increase in educational attainment there was a 24% (95% CI 21-27%) reduction in cardiovascular disease. Our MR analysis suggested a causal, protective effect for education against cardiovascular disease.
Association of education with mental health
We also found that education has an inverse association with anxiety and depression and that this is consistent across both adjusted observational and MR analyses (see Figure 2). For each standard deviation increase in educational attainment there were 25% (95% CI 24-26%) and 21% (95% CI 19-23%) reductions in depression and anxiety respectively. Our MR analysis suggested that education has a causal, protective effect against anxiety and depression.
Educational attainment generally showed only weak evidence of an association with mental health problems in our observational analysis (OR 0.99, 95% CI 0.98-1.01, p=0.06) but, in our MR analysis, there was evidence of a causal, protective effect (IVW OR 0.95, 95% CI 0.94-0.96, p<0.0001). This association was consistent across the MR sensitivity analyses.

The association of educational attainment with mental health and cardiovascular disease presented as odds ratios per standard deviation increase in education
Association of mental health with cardiovascular disease
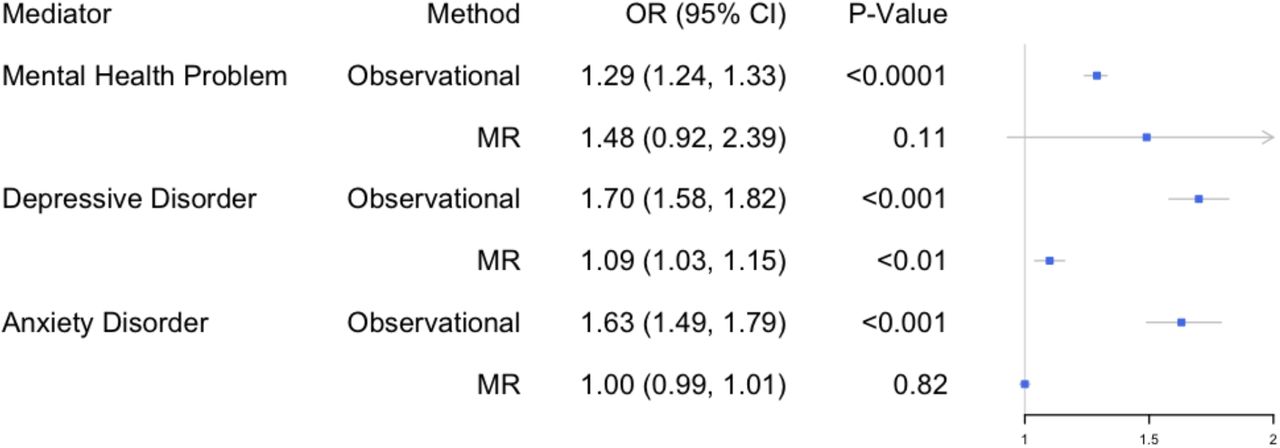
In our observational analysis, mental health problems in general were associated with increased cardiovascular disease risk (OR 1.29, 95% CI 1.24-1.33, p<0.001), but our MR analysis did not provide clear support for a causal interpretation (OR 1.48, 95% CI 0.92-2.39, p=0.11) (see Figure 3).
However, we found strong observational evidence that depression was associated with increased cardiovascular risk (OR 1.70, 95% CI 1.58-1.82, p<0.001), and our MR analyses supported a causal interpretation (OR 1.09, 95% CI 1.03-1.15, p=0.0021). Anxiety disorder was strongly associated with cardiovascular disease in our observational analysis (OR 1.63, 95% CI 1.49-1.79, p<0.001) but MR analysis did not support a causal interpretation (OR 1.00, 95% CI 0.99-1.01, p=0.82).
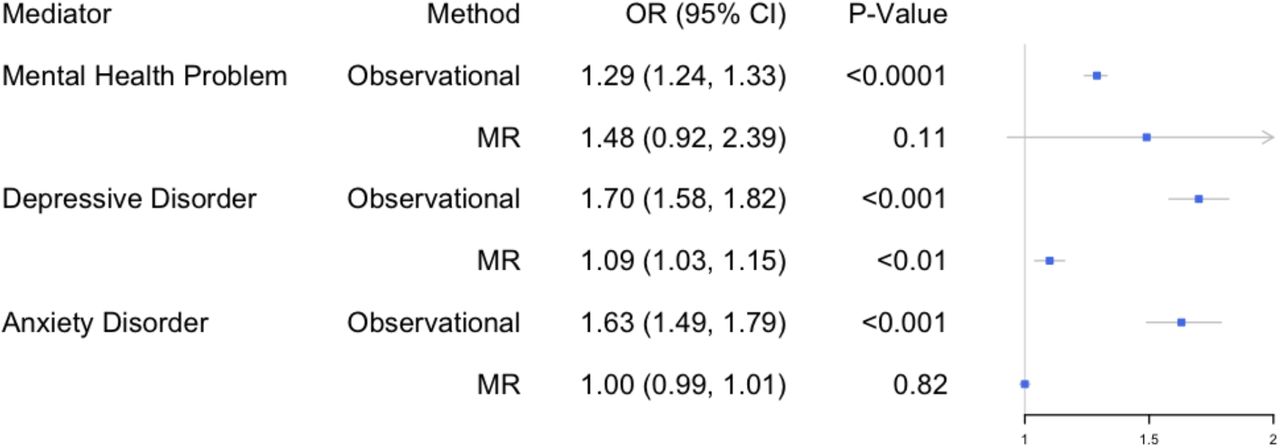
The association of mental health with cardiovascular disease following adjustment for the effects of educational attainment
Proportion mediated by mental health of the association between education and cardiovascular disease
Our mediation results show that mental health problems in general (2-step MR: 4.2%, 95% CI 3.0%-5.3%) and specifically depression (2-step MR: 6.5%, 95% CI 5.6%-7.5%) account for a small proportion of the negative association between education and cardiovascular disease (see Figure 4). The proportion mediated by anxiety disorder was very small in the observational analysis, and we found little evidence of mediation in our MR analysis.

The estimated proportions of the inverse association between education and cardiovascular disease accounted for by mental health presentations, depression and anxiety
Sensitivity analyses
The results of our sensitivity analyses are presented in Supplementary Tables S3-13 and included: testing for pleiotropy and reverse causation, testing for bidirectionality in our observational data, and testing personality traits as additional potential mediators. The results provided little evidence of bias from directional pleiotropy but did raise the possibility of reverse causation between cardiovascular disease and the proposed mediators in our observational analyses.
Exploratory analysis of tobacco smoking as a mediator between depression and cardiovascular disease
In a further analysis, we sought to investigate a potential role for multiple mediators in this pathway, specifically smoking as a mediator between adjusted depression and cardiovascular disease. We found that depression is associated with increased smoking activity and that lifetime smoking was associated with increased cardiovascular risk (see Supplementary Tables S15-16). In Figure 5, we show that smoking accounts for a large proportion of the increased cardiovascular risk associated with depression, 29% (95% CI 28.9-29.7%) according to our MR analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The estimated proportion of the association between depression and cardiovascular disease accounted for by lifetime smoking
Discussion
In this study, we used both observational and MR techniques to investigate mental health as a mediator between education and cardiovascular disease. Our results demonstrate that depression accounts for a proportion of the protective effect education has on cardiovascular disease.
We demonstrated, in observational analyses, that educational attainment has a clear, inverse association with anxiety disorder, major depressive disorder, and cardiovascular disease. Our MR analyses suggested these relationships are causal. In addition, our MR analyses suggested a causal, protective effect of educational attainment on mental health problems more broadly although observational analysis showed no strong association.
Mental health problems in general and, specifically, anxiety and depression were all associated with increased cardiovascular risk in our observational analyses. Our MR analyses only suggested a causal relationship between depression and cardiovascular disease.
Following these initial results, we further explored the proposed causal relationships between education, mental health and cardiovascular disease, which likely consists of additional mediators (see Figure 1). Our observational analyses showed that depression was positively associated with lifetime smoking which was, in turn, associated with increased cardiovascular risk even after adjustment for depression. Our MR analyses suggested these associations are causal. We found that lifetime smoking accounts for as much as 30% of the association between depression and cardiovascular disease.
Our results in context
Our analysis suggests that depression serves as a mediator between education and cardiovascular disease, and thus accounts for an unexplained portion of the protective effect of education. Specifically, it suggests that educational disparities may produce additional cardiovascular disease burden partly by increasing rates of depression. Depression and coronary artery disease have previously been found to be associated in MR work33,34; however, this mediation analysis constitutes a novel finding that can help identify possible new targets for interventions.
Our results support a protective role for education against mental health problems and, specifically, major depressive disorder and anxiety disorder. The foremost explanation for this is educational attainment being a proxy for overall socio-economic position which has a robust negative correlation with depression and anxiety35. For example, educational attainment is associated with both higher income and better occupation later in life 36,37. Such factors protect against experiences such as debt, financial struggles, and poor working conditions which feature amongst several relevant risk factors for mental health disorders38. Related interventions would accordingly include policies to promote educational attainment and reduce socio-economic inequalities.
At an individual level, further years spent in education or training are also likely to play a protective role against mental health problems by directly modifying a range of psychosocial factors and providing resources that can be drawn upon as stressors are encountered39. Such resources might include mental health advice, support networks, social participation, close friends, and good work-life balance40,41. Additional years in education may also help to offset exposure to stressors until one has greater maturity and resources to cope with them. By considering these observations, successful individual-level interventions in the education system might be developed.
In an exploratory analysis, we found that smoking accounts for a large proportion of the association between depression and cardiovascular disease. The link between smoking and cardiovascular disease is well-known and depression and smoking are also associated42,43. This link between smoking and depression has been commonly attributed to a ‘self-medication’ hypothesis where smoking is used to cope with depressive symptoms. Other factors that are proposed to partially explain the remainder of the association between depression and cardiovascular disease include chronic inflammation and changes in lipid metabolism44.
Implications
Our study has several important public health implications. First, it strengthens the case for investment in education and interventions related to it by demonstrating that educational attainment can reduce mental health burden, which is itself a significant source of morbidity and mortality45. Second, by illustrating the links between education, mental health, and cardiovascular disease, we have reinforced the need to recognise the potential interplay between social determinants, physical and mental health problems. Indeed, in this study, we show how a physical disease burden could be partly alleviated by targeting a social determinant of mental health. Finally, we have also illustrated how to further explore potential mediators between depression and cardiovascular disease in order to elucidate additional intervention targets. Here, we have highlighted tobacco smoking as such a target.
Strengths and limitations
The strengths of our study include the use of MR analysis to complement a conventional observational approach which allowed us to better overcome bias arising from confounding, measurement error and reverse causation. The use of a ‘triangulation approach’ also allowed for greater confidence in causal inference when there was consistency between the different approaches46. We were also able to limit bias arising from self-reporting and misclassification by using strict case definition for both our observational and MR data sources. Such bias can be particularly problematic when using binary exposures in MR47. An additional strength of our study was the use of two-step MR for a mediation analysis. This allowed us to specifically quantify the proportion of our exposure’s effect attributable to our proposed mediators. Finally, we extended our analysis in order to illustrate how our methodology could explore multiple mediators in the proposed pathway.
In our study, the use of MR demonstrated a discrepancy when observing the effects of mental health on cardiovascular disease. When adjusting for confounding in our mediation analysis, we likely over-adjusted in order to confidently isolate the effects of the mediator. To measure this, we conducted a sensitivity analysis without adjustment although this suggested that the effect sizes we have found may actually be underestimates (see Supplementary Table 17). Instead, the discrepancy may have primarily been due to reverse causation, with cardiovascular disease leading to mental health problems and exaggerating observed associations. In a further sensitivity analysis, where cardiovascular disease was the exposure and depression and then anxiety the outcomes, we did indeed find such bidirectionality.
A common limitation of MR studies is weak instrument strength48. Our instruments for both educational attainment and depression were adequate in this regard, with large mF statistics and sample sizes. However, our instrument for anxiety had a relatively smaller mF statistic and required a relaxed genome-wide significance threshold; the null result should therefore be interpreted with caution. However, we utilised the MR RAPS method to compensate for the relaxed threshold and we also conducted a sensitivity analysis with the worry sub-scale of the Eysenck Personality Questionnaire (Revised Short form). This analysis had adequate instrument strength and a larger sample size but also produced a null result (see Supplementary Table S8).
Despite adequate instrument strength, our ‘mental health problems’ instrument produced wide confidence intervals, suggesting these analyses may have been underpowered. Unlike our other instruments, this one was constructed from a GWAS performed on a single sample, as the unusual phenotype measured is only available in the UK Biobank. In future, we hope other cohorts will have this or a similar phenotype measured, leading to larger sample sizes for analysis and, hopefully, the discovery of further significant variants.
When conducting two-sample MR, overlap between the samples can be problematic. The samples used for our exposure and mediators did feature partial overlap due to the use of UK Biobank data in both sets. This introduces a greater risk of a type I error in our two-sample univariable analyses of education and mental health due to possible overfitting. However, we also saw an inverse association with education in our sensitivity analyses that utilised personality traits related to mental health (see Supplementary Table S8). These featured substantively less overlap between samples. In addition, this limitation did not apply to our two-step analysis which pools the data for the exposure and mediators before analysis is conducted.
Another common limitation of MR studies is bias from directional pleiotropy49. We conducted numerous sensitivity analyses, including multiple MR methods and measurement of MR Egger intercepts (see Supplementary Tables S3 and S7), which suggest our results were not biased by directional pleiotropy.
Finally, even with our approach, education may still be acting as a proxy for socioeconomic position. A proposed strategy for investigating this would be to conduct an additional analysis using a measure such as household income which would allow for comparison as well as adjustment as part of a multivariable MR approach. A recently published GWAS meta-analysis exploring household income50 offers the possibility of this in future studies. Natural experiment techniques could also be used having previously suggested that the raising of school age reduced cardiovascular disease51.
Conclusions
In conclusion, we have demonstrated that educational attainment is inversely associated with mental health problems, anxiety, depression, and cardiovascular disease. A reduction in depression accounts for part of the inverse association between education and cardiovascular disease. Finally, we have shown that smoking accounts for a large proportion of the association between depression and cardiovascular disease. Our findings offer significant clinical and public health implications by further demonstrating interplay between social determinants, mental and physical disease and associated targets for intervention.
Data Availability
The data used for the observational analyses conducted in this study is available to qualified researchers upon application to the UK biobank (https://www.ukbiobank.ac.uk/researchers/). The data used for the MR analyses conducted in this study is publicly available via the cited references.
Sources of Funding
REW, HMS, ARC and MRM are all members of the Medical Research Council (MRC) Integrative Epidemiology Unit at the University of Bristol funded by the MRC: http://www.mrc.ac.uk [MC_UU_00011/7]. DG is supported by the Wellcome Trust 4i Programme (203928/Z/16/Z) and British Heart Foundation Research Centre of Excellence (RE/18/4/34215) at Imperial College London. This study was supported by the National Institute Health Research (NIHR) Biomedical Research Centre at the University Hospitals Bristol National Health Service (NHS) Foundation Trust and the University of Bristol. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Disclosures
DG is employed part-time by Novo Nordisk. No other conflicts of interest and no further funding sources are declared.
Supplementary Materials
Supplementary Methods
Supplementary Tables S1-S15
Supplementary Figures S16-S17
References 52-571
Acknowledgements
We are grateful to the participants of the UK Biobank and the individuals who contributed to each of the previous GWAS analyses conducted as well as all the research staff who worked on the data collection. This research has been conducted using the UK Biobank Resource under Application Number 9142.
References




