
Abstract
Background Emergence of new multisystem inflammatory syndrome in children (MIS-C) is thought to be associated with COVID-19 pandemic. Covid-19 morbidity and mortality variances among countries has been suggested by previous works to be influenced BCG and previous Latent TB infection (which is reflected by TB prevalence) by possible inducing heterogeneous immunity against SARS-COV2.
Aim To examine influence of BCG status and TB prevalence on variances among countries which register new multisystem inflammatory syndrome in children (MIS-C).
Methods We choose all countries which report MIS-C till 23/6/2020, number of cases for each 10 million capita was examined among 3 categories of countries classified according to BCG program status. TB prevalence, MIS-C no. / 10 million (M) and Covid-19 deaths/M are taken as markers. Receiver operation characteristic - (ROC) curve, as well as some relative indicators such as (sensitivity and specificity rates), estimation area of trade - off between sensitivity and specificity, and cutoff points are used for discriminating different three pairs of countries (which have different BCG practices). Discrimination of these categories done through studied markers. 95% confidence interval of all probable combinations pairs had been measured.
Results MIS-C No/10 M capita in countries never gave BCG vaccination vs countries currently give vaccine shows area under ROC-curve equal to 0.000 with a symbiotic significant of 0.034 and (95% CI interval of 0.000-0.000) also MIS-C No/10 M capita in countries not currently give BCG vaccination (with previous mass vaccination programs) vs countries currently give mass vaccination shows area under ROC-curve equal to 0.094 with a symbiotic significant of 0.027and (95% CI interval of 0.000 -0.280)
Important not significant finding in MIS-C No/10 M capita in countries never gave BCG vaccination vs countries not currently give vaccine shows area under ROC-curve equal to 0.583 with a symbiotic significant of 0.683 and (95% CI interval of 0.074-0.759). Countries not currently give vaccine make discrimination in other pairs
COVID-19 deaths M capita in countries never gave BCG vaccination vs countries currently give vaccine shows area under ROC-curve equal to 0.083 with a symbiotic informative and reportable value of 0.077 and (95% CI interval of 0.000-0.309 also COVID-19 deaths M capita in countries not currently give BCG vaccination vs countries currently giving vaccine shows area under ROC-curve equal to 0.188 with a symbiotic informative reportable value of 0.089 and (95% CI interval of 0.000-0.452).
Important finding is the not significant association in COVID-19 deaths /M capita in countries never gave BCG vaccination vs countries not currently giving vaccine area under ROC-curve equal to 0.417 with a symbiotic significant of 0.683 and (95% CI interval of 0.078 - 0.755). Countries not currently giving vaccine make discrimination in third pair of countries in significant association and not in 1st pair.
Regarding TB prevalence marker or discriminator the areas under curve were informative and reportable and too generating with the leftover markers in all 3 pairs signifying inverse relations with covide-19 mortality and MIS-C no. curves.
Conclusion BCG vaccinations and high TB prevalence are found in this study to be related to decrease MIS-C and COVID-19 deaths this might explain variances among countries worldwide. Further studies to confirm this relations and possible relations with other epidemics is recommended. Review of TB programs in relation to treat latent asymptomatic infections and initiate and consolidate BCG programs should be considered urgently.
Introduction
In April of 2020, reports emerged from the United Kingdom of a presentation in children similar to incomplete Kawasaki disease (KD) or toxic shock syndrome1, 2,3. In Italy, approximately 10 suspected Kawasaki-like disease cases have been recorded since 1 January 2020, eight of which were reclassified as new Paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 infection in children (PIMS-TS)4 or multisystem inflammatory syndrome in children (MIS-C) or paediatric hyper inflammatory syndrome, or paediatric hyper inflammatory shock1. Classical KD with concurrent COVID-19 also have been reported5. MIS-C is hyper inflammatory syndrome with multiorgan involvement have some features similar to those of Kawasaki disease and toxic shock syndrome (KDSS)6.
(KD) is an acute febrile systemic vasculitis that predominantly occurs in children younger than 5 years of age and the most common acquired heart disease during childhood in most industrialized countries7 and is the most common primary vasculitis in childhood, with medium and small sized arteries predominantly affected8. The annual incidence of KD is highest in Japan, with more than 300 per 100□000 children aged 4 years or younger affected9, compared with 25 per 100□000 children aged 5 years or younger in North America10and is rarely reported in sub-Saharan Africa11. Although KD is less common in western countries 12 KD shock syndrome (KDSS) a rare form of KD has a higher incidence in these countries 13 (2.60 to 6.95%)14,12,15, compared with Asian countries like Taiwan which reported lower incidence rate (1.45%)16.
KDSS is often associated with myocarditis and requires critical care support during the acute phase of illness KDSS might mimic toxic shock syndrome12.
A high level of circulating pro-inflammatory cytokines might contribute to the distributive component of shock. Indeed, KDD has been found associated with high levels of IL-6,, and procalicitonin13.Patient with MIS-C also high levels of inflammatory markers, including leucocytosis with a predominance of neutrophils, in addition to high levels of C reactive protein, ESR, procalcitonin, and serum interleukin 617. Furthermore elevation of inflammatory markers (cytokines) has been previously demonstrated in inflammatory state for multiple conditions18including cytokine storms. Cytokine storm denotes a hyperactive immune response characterized by the release of interferons, interleukins, tumor-necrosis factors, chemokines, and several other mediators. These mediators are part of a well-conserved innate immune response necessary for efficient clearance of infectious agents. Cytokine storm implies that the levels of released cytokines are injurious to host cells19,20. Cytokine storms can be caused by a number of infectious, especially viral respiratory infections such as H5N1,H1N1 influenze and SARS-CoV21,22 Other causative agents include the Epstein-Barr virus, cytomegalovirus23. Likewise in KD circumstantial evidence points to an infectious cause24. In the past 20 years, viruses of the coronavirus family have been proposed as possibly implicated in the pathogenesis of Kawasaki disease.25,26
It is said that case definition of MIS-C is quite broad and overlaps with Kawasaki disease, and other conditions like juvenile rheumatoid arthritis27. On the contrary some experts are concerned that current diagnostic criteria may not capture the true scope of the problem.28
The severity of inflammation in KD is reflected by inflammatory parameters; thus, laboratory findings are helpful for diagnosing incomplete KD just like MIS-C. A child is considered to have incomplete KD when there are fewer than 4 clinical features in the presence of fever1. “Atypical KD” should be used in the presence of an unusual or odd manifestation of KD (e.g., nephritis or central nervous system complication)29. Incomplete KD is considered to be a mild form of KD30. Nevertheless, such children may have significant coronary artery sequelae as the diagnosis and treatment are often delayed31.
Differences in Kawasaki shock syndrome and MIS warrants studies investigating underlying immunological mechanisms. Kawasaki disease in its milder form is prevalent in Asian countries. Furthermore, sever form of KDSS, sever covid-19 and MIS-C observed in western countries while milder in Asian and sub-Saharan Africa.
Cardiac manifestations in MIS might mimic Kawasaki or Kawasaki shock syndrome and include myocardial dysfunction, pericarditis, valvulitis, or coronary abnormalities other clinical features may overlap.
Reactivation of the Bacillus Calmette–Guérin (BCG) injection site has been listed by the American Heart Association as a significant finding among the diagnostic guidelines for KD32. Such finding might account to 50%of patients33,34. In spite of that no study done before to show BCG effectiveness in KD disease process. BCG reactivation is thought to happen due to suggested cross reactivity of mycobacterial Heat Shock Protein 65 (HSP65) and the human homologue HSP63. Furthermore, cross immune heterogeneity was suggested between BCG and many viral diseases and neonatal sepsis. Since early months of covid -19 pandemic and forward literatures suggest the role of BCG in decreasing the severity and mortality of COVID-19 and possibly morbidity. Furthermore, annual a symptomatic latent TB infection might play a natural role like BCG in protecting communities with high TB prevalence.
Epidemiological studies are lacking regarding role of BCG or latent TB protection effect on incidence of MIS-C and KDSS in addition to KD.
This study is the first in this aspect handling MIS-C incidence in relation to BCG, TB prevalence and COVID-19 deaths.
At early times during COVID-19 pandemic heterogeneous immunity towards (SARS-CoV-2), was hypothesized and statistical correlation between of (BCG vaccination practices and TB prevalence) and COVID-19 mortality among countries was statistically confirmed. They suggest that BCG (attenuated Mycobacterium bovis) and possibly previous latent or active TB caused by Mycobacterium tuberculosis) have heterogeneous immunity to certain pathogens other than Mycobacterium tuberculosis effect.
As far as Mycobacterium bovis through BCG has heterogeneous effects to various microorganisms and possibly to SARS-COV2 and possible relation of low TB prevalence to high covid-19 mortality I put the question of this paper in such way : if BCG programs and TB prevalence affects MIS-C morbidity. This study might gain its importance because of no study was done about MIS-C relation to TB prevalence or BCG vaccination and to possible relation between them. This might open the door to furtherly identify relations with KDSS, KD or other hyperimmune serous conditions.
Material and Methods
Data regarding to MIS-C collected till 23/6/2010 in all countries which register MIS. Then Covid-19 deaths/Million registered as it appeared on public data accessed on 2/7/2020. Countries BCG practices were put in three different groups :
No vaccination at all and no previous BCG
no current vaccination but with previous vaccination program (ceased BCG vaccinations previously), and
currently giving mass BCG vaccine through national program.
Total countries were 15, distributed among that groups status as shown in table No. (1). Covid -19 mortality, data TB prevalence data, and population data are obtained from publically published data. BCG data are obtained from publically available WHO data and various references.
MIS-C No./10M, Covid-19 deaths/Million versus BCG practice group of countries
Receiver operation characteristic - (ROC) curve, as well as some relative indicators such as (sensitivity and specificity rates), and cutoff points are used for discriminating different three categories of countries (which have different BCG practices).
Discrimination of these categories done through studied markers. All statistical operations were performed through using the ready-made statistical package SPSS, ver. 22.
Results and Findings
Table 1 shows collected data for the study sample in terms of country No. of cases, BCG status, Covid-19 deaths and TB prevalence.
Group 1 (No vaccination at all no previous BCG) shows highest mean value for COVID-19 deaths/M and lowest of TB prevalence
Group 3 (Currently giving BCG vaccine) show lowest MIS-C no./M and lowest COVID-19 mortality and highest TB prevalence.
Group 2 No current vaccination (previous vaccination) group shows highest MIS-C and other parameters was in between.
We present the results of each BCG status pair for the three BCG groups :
Table No. (2) shows estimates area of trade - off between sensitivity and specificity of markers through plotting sensitivity against a complement specificity outcome to examine that trade - off, which is called (ROC) curve, as well as a significant level for testing area under the guideline of fifty percent, with 95% confidence interval of all probable combinations pairs of countries as follows:
Relationships among a diseased groups & controlled for all probable combinations of Disclusion time test in different parameters
Pair of countries with no vaccination program at all (x axis) & no current vaccination program but have previous vaccination program (y axis):
The common think in this pair is that both groups had no vaccination programs at this time whether had previous history of vaccinations or not.
Pair of countries with never gave BCG vaccination program (x axis) & those with currently giving BCG vaccination (y axis).
Pair of countries with currently no vaccination (ceased vaccination program) (x axis) & currently vaccinated (y axis).
Findings are
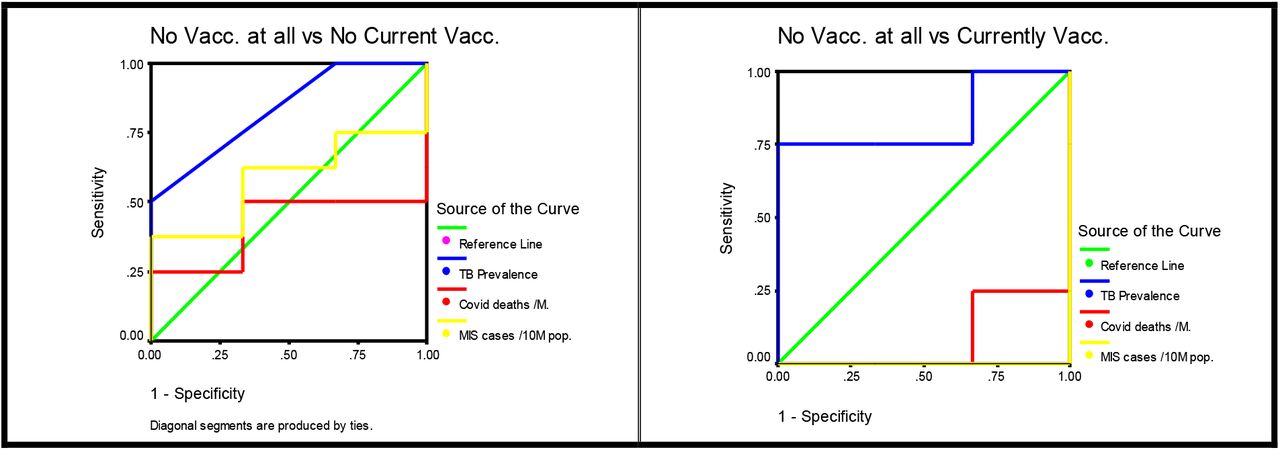
Findings are : MIS-C No/10 M capita in countries never gave BCG vaccination vs countries currently giving vaccine (pair 2) shows area under ROC-curve equal to 0.000 with a symbiotic significant of 0.000 and (95% CI interval of 0.000-0.000) also MIS-C No/10 M capita in countries not currently give BCG vaccination(ceased mass vaccination programs) vs countries currently give mass vaccination (pair 3) shows area under ROC-curve equal to 0.094 with a symbiotic significant of 0.027and (95% CI interval of 0.000 - 0.280)
Important not significant finding in MIS-C No/10 M capita in countries never gave BCG vaccination vs countries not currently giving vaccine (1st pair) shows area under ROC-curve equal to 0.583 with a symbiotic significant of 0.683 and (95% CI interval of 0.074-0.759) countries not currently giving vaccine make discrimination in 2nd pair of countries in significant association and not in 1st pair.
COVID-19 deaths M capita in countries never giving BCG vaccination vs countries currently giving vaccine (pair 2) shows area under ROC-curve equal to 0.083 with a symbiotic informative and reportable value of 0.077 and (95% CI interval of 0.000-0.309 also COVID-19 deaths M capita in countries not currently giving BCG vaccination vs countries currently giving vaccine(3d pair) shows area under ROC-curve equal to 0.188 with a symbiotic informative reportable value of 0.089 and (95% CI interval of 0.000-0.452)
Important finding is the not significant association in COVID-19 deaths
/M capita in countries never giving BCG vaccination vs countries not currently give vaccine (1st pair) shows area under ROC-curve equal to 0.417 with a symbiotic significant of 0.683 and (95% CI interval of 0.078 - 0.755). Countries not currently giving vaccine make discrimination in third pair of countries in significant association and not in 1st pair.
Regarding TB prevalence marker or discriminator the areas under curve were informative and reportable and too generating with the leftover markers in all pairs and were 0.833 with 59% CI of 0.572-0.755 in pair one and 0.833 with 95% CI interval of 0.5-0.500 and 0.750 with 95% CI interval of 0.326-1.174 in pairs 2 and 3 respectively. These signifying inverse relations with covide-19 mortality and MIS-C no. curves. The informative reportable asymptotic values were0.102,0.157,0.174 for 3 pairs respectively.


{kind=link}
{kind=link}
represented graphically of ROC Curve plots for studied markers in relative with BCG practices in pair’s combinations in light of different three categories conditions.
In order to create a cut-off points for the markers searched between the three pairs of classifiers in relative with BCG practices, and some screening tests such as sensitivity, and specificity rates are presented in table No. (3).
Estimation of sensitivity, specificity rates and construct a cutoff points between different three categories of BCG vaccine due to studied markers
Results shows that MIS-C cutoff points seems to be inconsistent for the three pairs with too increase for the third pair and lowest in 1st pair.
It is clear that TB prevalence cutoff points are more in 3d pair then 2nd pair both of these pairs have current countries with BCG vaccination programs.
Discussion
Significant positive relations between BCG status with COVID-19 deaths and MIS-C rates as is shown in ROC-Curves. TB prevalence is also significantly associated with similar influence like BCG.
Regarding MIS-C there is strong relations with BCG status being effective in decreasing incidence in countries currently give BCG vaccine with partial effect on those with previous vaccination programs. countries never gave BCG vaccine being mostly affected.
Literatures previously suggest that BCG have such beneficial effect of BCG lowering COVID-1935 mortality, our findings consolidate previous findings.
It is obvious that MIS-C was first thought to be KD or KDSS as health authorities in the United Kingdom reported a number of seriously ill children presenting with signs of circulatory shock and hyper inflammatory state, with features consistent with toxic shock or KD on 27 April 2020. Some of the tested children were positive for SARS-CoV-2 infection. Austria, Greece and Sweden reported not seeing an overall increase in cases of KD. No increase was observed in Asian countries, where KD is much more prevalent than in Europe, such as Japan and South Korea till now. France and Italy observed an unusually high number of children with TSS (with some features reminiscent of KD) in pediatric intensive care; some of those children also tested positive for SARS-COV-24. Even after IMS-C diagnostics criteria have been developed by Royal College of Paediatrics and Child Health (RCPCH) 36 Centers for Disease Control and Prevention (CDC) 37 and World Health Organization (WHO)38 there differences in each criterion nevertheless some believe these criteria are broad overlaps with many conditions like Kawasaki disease,27 others believe these capture the true scope of the problem.28
Till 23/6/2020 nine countries reported MIS-C even though many other countries continue to report further. News of confirmed or suspected cases has since emerged from several other countries, including Russia39, India40, Pakistan,41 Iran,42 Israel43, and Algeria44.In Southeast and East Asia, no apparent increase in cases Kawasaki disease was reported4.
KD occurred with relatively constant but slowly growing rates. The appearance and subsequent incidence of KD may be associated with the time of industrialization and westernization of these countries45. Therefore, it could be postulated that in the past, KD (infantile polyarteritis nodosa) might have appeared in Western countries around the beginning of the 20th century46. Recently, clinical features of KD seem to be changing to milder phenotypes with greater numbers of incomplete KD cases47.
From the first patient with KD reported in 1961 and the 50 patients published in 1967 by Dr. Tomisaku Kawasaki over the following 5 years48
KD is thought to be as one of diseases with excessive immune system response to possibly viral infection 49. Its incidence of KD (per 100,000 less than 5-year-olds) of Kawasaki disease by country50 in decreasing order of incidence : Japan 308 in 201451, South Korea 194.7-217.2 in 201452,53, china 72.03 in 1.9-116.6 in 2012-201450,54, Taiwan 82.8 in 201055, Canada 19.6 in 201456,United States19.1 in 201550,Italy 14.7-17.6in 201357,58, Finland in 11.4 in 200959, Chile 10.4 in 201160, Australia 9.34 in 200961, France 9 in 2005-2006, Spain 8 in 201462, Inner Mongolia 7.7 in 201363, Sweden 7.4 in 200959, Germany7.2 in 201264, Portugal 6.5 in 201165, Netherland 5.8 in 201266,united kingdom 4.55 in 2013-201567,Thailand 3.43 in 200268, Israel 2.03 in 201269. In Latin America the incidence of KD has been reported sporadically in several countries60,70. Many nations around the world have demonstrated an increase in the number of children diagnosed with KD since the early to mid-2000s.71
In the view of absence of stationary incidence of Kawasaki-like multisystem inflammatory syndrome associated with SARS-CoV-2 infection in Asian countries where the covid-19 pandemic started, and where the incidence of Kawasaki disease is the highest, is noteworthy72. Identifying of factors lead to increase incidence KD in Asia and factors lead to increase of KDSS and KD like illness in Europe and USA should be analyzed in contex of recent development of Kawasaki like disease ie IMS-C with special consideration to outbakes of KD or KD like illnesses in temporal relations to epidemics and outbakes. Analyses should go retrograde to look for possible epidemiological links to look for evidence of such temporal associations.
In 1918 pandemic although cytokine storm was hypothesized but no report or for Kawasaki or Kawasaki like syndrome 1918 pandamic, but some analyses have shown the virus to be particularly deadly because it triggers a cytokine storm, which ravages the stronger immune system 73.
Since that time literature research on the impact of Spanish influenza does indicate that the Chinese people survived much better than people in the USA and Europe74. Even so some patients in China were complicated with bronchitis, pneumonia, and even hemolysis. Erythema was found in some patients were usually misdiagnosed as scarlet fever74 .Rashes might be a very rare flu sign anyhow skin manifestations makes one aware of possible Kawasaki or incomplete Kawasaki in china there before KD disease definition later on. According to Dr A. Stanley who was employed by the Shanghai Health Bureau at that time in some cases unfortunately these rashes were usually misdiagnosed as scarlet fever74. Anyhow rash could be associated with influenza A and typically macular or maculopapular in nature and occurs in about 2% of patients —usually children75.Furthermore during 2009 pandemic Influenza virus rash is uncommon, and a rare cause of petechial rash in severely affected children were described76. According to that the rash associated to Chinese patient more likely is rash of Influenza A as to Dr A. Stanley said rather than to disease related to Kawasaki or Kawasaki like.The low mortality and morbidity among Chinese people were attributed to Chinese herbals74.
In western countries it looks that the pandemic was sever. To maintain morale, World War I censors minimized reports of pandemic in France (Brest), Germany and the United Kingdom and USA77.
The major UK troop staging and hospital camp in Étaples in France has been theorized by virologist John Oxford as being at the center of the Spanish flu 78 His study found that in late 1916 the Étaples camp was hit by the onset of a new disease with high mortality that caused symptoms similar to the flu and according to Oxford, a similar outbreak occurred in March 1917 at army barracks in Aldershot78,79, 80.Military pathologists later recognized these early outbreaks as the same disease as the 1918 flu78,81.Furthermore published data from the Austrian archives pointing that the Spanish influenza in Austria began in early 191782. It is of forth mention to say that a disease thought to be measles appeared in 1917–18 produced the highest infection rates in 97 years of continuous military surveillance83 and extreme case-fatality from aggressive bronchopneumonias and other complications84. For reasons that were unclear, infection rates were highest in some camps .Severity statistics were striking: 95 843 measles cases occurred, 22 809 (23·8%) people were admitted to hospital for complications, and 3206 (3.34%) people died. At Camp Pike (Little Rock, AR) they thought that this measles is thought to have killed more soldiers than the 1918 influenza pandemic84. These findings make me think that MIS-C like disease might be back to 1917 due to possible relation to H1N1 spanish flu in mechanisem similar to what happens now with SARS-COV2, specially these bronchopneumonias showed similar streptococcal pathological changes and seem to have been associated with previous respiratory viral infections85,86presumably including seasonal influenza and other viruses84.Some of these deaths documented not only specific to postmeasles pneumonias because an epidemic of severe and fatal primary pneumonia or empyema, or both, in soldiers without measles, which paralleled the measles case-fatality rather than measles incidence84.
The preeminent pathologist of the camp epidemics, Johns Hopkins’ William MacCallum (1874–1944), coined the term interstitial bronchopneumonia to describe 1917 measles (and later, 1918 influenza) autopsy findings84,87,88.
In recent MIS-C pandemic skin rash is common in more than half reported rash, as the NYC Health Department said89.
Tuberculosis mortality was in decline in the US since at least the mid-nineteenth century. The overall decline was greatly thought to be accelerated by the 1918 pandemic, but as far as the process would have continued, albeit more slowly, even if the 1918 pandemic had not occurred90 make me think that the decrease in TB is possibly related to high mortality and complication due to Spanish flue rather than opposite explanation although this should be documented .Here in this paper we show that both TB prevalence and BCG status have influence on both covid-19 mortality and MIS-C incidence. Is TB through latent or previous infection or through BCG vaccination has cross immunity protection against covid-19 pandemic and other influenza pandemics making these pandemics more sever in western countries and such severity affect adults and children. Is it probable that when TB prevalence starts to decrease in Asia some sort of hyper immune condition emerges in susceptible children and this took the form of KD or incomplete Kawasaki?? In Japan Large-scale influenza epidemics have occurred in the past, including the Spanish flu during 1918–1920, Asian flu during 1957–1958, Hong Kong flu during 1968–1969, and 2009 H1N1 pandemic during 2009–2010.
Japan currently giving BCG and stop boosters since 2003 and have previous TB programs. The Ministry of Health and Welfare in Japan conducted the first National Tuberculosis Survey in 1953, and found more severe endemic status than expected. In order to improve this situation, “Guidelines for Strengthening of Tuberculosis Control Measures” were issued in 1954 furthermore developments in medical science for TB treatment, particularly the development of chemotherapeutics, had a big impact on TB control91. TB was transformed from a fatal to a curable disease and by 1961 the mortality rate from TB dropped sharply furthermore compulsory vaccinations started at 1948 as national policy91. By the 1950s, the first effective antimicrobial drugs against TB (i.e., streptomycin, para-amino salicylic acid, and isoniazid) had been developed. This help in reducing the prevalence of TB in many countries92.
Up to my knowledge there is no study done to answer the question of sudden drop of TB prevalence to emergence of Kawasaki disease in Japan or to study the low rate of KDSS compared to Europe which most of countries have low TB prevalence and variations in BCG program practices. According to our work we find a influence of BCG vaccination on covid 19 deaths and IMS-C in a strong relation experts are looking for increase in KD in Asian countries at this time, but this might needs time according to history of previous epidemics and outbakes.
In japan the major peak in influenza cases in 1957 represents the country’s first exposure to the H2N2 subtype, which caused the 1957 Asian flu pandemic which is a new influenza A (H2N2) virus emerged in East Asia, triggering a pandemic. The quite extensive outbreaks in 1962 and 1965 were due to H2N2 variants that arose from antigenic drift93
13 outbreaks of swine influenza were recognised in Japan from 1978 to 1979. Thirty-seven influenza viruses were isolated from nasal swabs of diseased pigs in 13 outbreaks. During the winter of 1978–79, the reappearance of the A(H1N1) virus coincided in some countries with epidemics of A(H3N2), and several instances of co-infection were reported in the United States and Japan94.
Furthermore influenza type B viruses were associated with increased morbidity widespread illness in schoolchildren in Japan in February 1982 95 were associated with increased morbidity in some regions of the Union of Soviet Socialist Republics (USSR) in November and December 1981.
The 1986-87 influenza epidemic was caused by influenza A(H1N1) viruses resembling A/Taiwan/1/86(H1N1), a variant first isolated in China, Malaysia, Japan, and Singapore during January-April 198696. Shortly after and on word and possibly temporarily associated with 4 previous out brakes of 1962 and 1965,1978-1979,1982, 1986, three large KD epidemics were recorded in Japan—in 1979, 1982, and 1986 in addition to the first reported by Tomisaku Kawasaki in January 1961, and his later report on 50 similar cases on 196748 just one year before 1968 flu pandemic.
The reported annual incidence rates of KD in Japan were 206.2 and 239.6 per 100,000 children aged 0 to 4 years in 2009 and 2010, respectively; the 2010 rate was the highest ever reported before. In 2009,a new influenza strain (H1N1) was prevalent worldwide, including Japan97.The influenza epidemic might have changed the epidemic pattern of KD. The influenza epidemic might have had an effect as suggested by Yosikazu Nakamura 1, Mayumi Yashiro, Ritei Uehara,etal97.The temporal associations of KD out brakes in Japan from 60s of last century till 2009 with concurrent virus out brakes is of great concern and the time is too early for japan to say there is no association with current pandemic.
In USA a community-wide outbreak of Kawasaki syndrome, apparently the first in the United States, occurred in Hawaii in the first half of 1978. According to CDC there were isolates of H1N1 in Hawaii in mid-February 1978 98.This temporal relation may be related to possible causative virus. Between August 22, 1984, and January 6, 1985, 10 outbreaks of Kawasaki syndrome (KS) Outbreaks occurred in 10 states and the District of Columbia during the 21-week period. Cases from a number of these outbreaks continue to be reported to CDC99 no research data were found to relate KD out brakes to outbreaks of type A(H1N1) strains during the 1983-1984 influenza season100 but the temporal association is evident.
In South Korea the incidence rates of KD just after 2009 influenza pandemic in children younger than 5 years increased from 115.4 per 100,000 children in 2009 to 134.4 per 100,000 children in 201153,52. The incidence furtherly increased to 170.9, 194.9 and 194.7 in 2012, 2013 and 2014, respectively53.TB prevalence in south Korea was 80 /100000 in 2011 decreased to 66 in 2018101. Compared to Japan South Korea have lesser incidence of KD and higher TB prevalence since South Korea start BCG at late times in 70s and stopping boosters in 2007102.
In China: the start and peak of Kawasaki epidemics in 1979, 1982, and 1986 these out brakes are coincidental to Japan’s for mentioned peaks of KD, furthermore seasonal outbreaks between 1987-2010 103.
The “flu” of 1979 originated in fact in mainland China in early 1977 which was caused by another “new” virus that is not new at all but which circulated widely in the early 1950’s, then vanished with the advent of “Asian” (H2N2) influenza in 1957104 furthermore Influenza A(H1N1) virus was isolated in China in 1982. According to CDC virus of this subtype has not previously been isolated.105 Although the prevalence of TB changed little from 134.27 in 1990 to 137.93 in 2015 per 100,000 persons106. TB prevalence again is higher than Japan might explain lower incidence of KD in China compared to Japan.
In Europe, the epidemiology of KD ranges from 3.6 to 15.2/100,000.107but (KDSS) has a higher incidence in these countries13,compared with Asian countries the real cause for high incidence of KDSS in western countries is unknown yet. Low TB prevalence and lack of BCG vaccination might put these countries to report higher rate of KDSS.
BCG is considered weak TB infection through Mycobacterium bovis present in vaccine and this have heterogeneous immunity with Mycobacterium tuberculosis furthermore immune heterogeneous effects extends to variety of viruses108 and possibly includes SARS-CoV-2109.
BCG unlike natural infection gives protection to 50%-60 %110 of target population. This might possibly have explained prevalence of KD when TB prevalence start to decrease in communities to relatively medium level of TB prevalence possibly due to presence of BCG vaccinations In contrast higher rate of KDSS are found in unvaccinated communities and lower TB prevalence although KD is lower than Asian countries. We found here in this paper higher incidence of IMS-C associated with low TB prevalence countries and associated with lack of BCG programs. The incidence of IMS-C vary within European countries possibly due to variations in BCG recommendations concerning its use in Europe as follows:111 there are 12 countries do not include it in their normal vaccination schedules (Austria, Belgium, the Czech Republic, Denmark, Germany, Iceland, Italy (start 1970 and stopped 2001) Liechtenstein, Luxembourg (stopped mass vaccination previously BCG coverage was 20% on 2005 and 60% on 1995-1998112), the Netherlands, Slovakia, and Spain); there are 11 recommend its use in all newborns at the time of birth (Bulgaria, Croatia, Estonia, Greece, Hungary, Ireland, Latvia, Lithuania, Poland, Portugal, and Romania), The remaining 8 (Cyprus, Finland, France stopped mass vaccination on 2004), Malta, Norway, Slovenia, Sweden, and the United Kingdom) recommend it only for certain categories of children considered at risk, mainly the children of parents coming from TB endemic countries and those with a case of TB in their families.
Recommendations
As far as this study shows a strong relation between BCG and MIS-C, between BCG prevalence and COVID – 19 deaths, and between TB prevalence and MIS-C and between TB prevalence and COVID-19 deaths so our recommendation is that BCG vaccination clinical trials are required to corroborate the patterns detected here, and to establish causality between BCG vaccination and protection from severe COVID-19 and possibly other epidemics.
Further recommendation is to review TB programs be more conservative in treatment of latent infections and revaccinate people with primary BCG vaccinations and further booster doses.
Data Availability
All relevant data are available on requist
There is no conflict of interest.
There is no funding received.
Acknowledgment
I am deeply grateful to Emeritus Professor Abdulkhaleq Abduljabbar Ali Ghalib Al-Naqeeb, Ph.D. in the Philosophy of Statistical Sciences at the Medical & Health Technology college, Baghdad-Iraq, for his assistance and supported in data analysis, interpretations of finding results, and revise and display the paper.
References




