
Abstract
Back ground Latent TB disease reflect a state of persistent immune response to stimulation by Mycobacterium tuberculois. TB infection lead to latent TB disease in 90-95 % while 5-10 % of individuals develop active TB disease when compared to BCG, BCG is 60% effective against the development of active TB. Studies done to test association of BCG with covid-19 morbidity and mortality and it was thought that BCG have preventive effects due to presumed non specific anti viral effects in this study we test association between prevalent of TB which reflects about 90-95 % of corresponding latent TB infection with covid 19 mortality.
Materials and methods countries divided into 5 groups according to BCG following status: No vaccination at all no previous BCG group, no current but had BCG in past (one or more), 1 current BCG with previous booster (s), just 1 BCG now no previous booster (s) and more than 1 BCG setting now. covid-19 deaths taken as it is on these are tested against TB prevalence 2018.
Results Slop values have significant influences between TB prevalence and covid-19 deaths among all tested groups and are reversed in just 1 BCG now no previous booster (s) group
P<0.01 coefficient (0.30751),1 current BCG with previous booster (s) P<0.01 coefficient (0.63662), and more than 1 BCG setting now group P<0.05 with coefficient of (0.61580). While no vaccination at all no previous BCG group shows Compound model linear regression P<0.05 coefficient (97.45%)and No current but had BCG in past (one or more) group shows Cubic model P<0.01, coefficient (66.098%)
The overall slope value is highly significant and reverse influence at P<0.01, as well as highly significant relationship coefficient (0.36749).
The linear regression model obtained in logarithmic mode for all tested sample and being inverse in countries with more than 1 BCG setting at this time and countries with 1 current BCG with previous booster (s) furthermore linear regression model is logarithmic in countries with just 1 BCG now and no previous booster (s).
Conclusion TB prevalence is strongly associated with covid-19 mortality and being more sever in absence of BCG vaccine.
Recommendations Early interventions might be considered based on the supportive evidence at this timewhich include BCG vaccination, review of current latent TB programs.
Introduction
About one-quarter of the world’s population may be infected with latent tuberculosis which1 is defined as a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifest active TB2. It is estimated that the lifetime risk of an individual with LTBI for progression to active TB is 5–10%3, furthermore more than 90% of people infected with M. tuberculosis for more than two years never develop tuberculosis even if their immune system is severely suppressed4,while BCG is highly efficacious at preventing meningeal and miliary TB, but is at best 60% effective against the development of pulmonary TB in adults and wanes with age.5 It is hypothesized that beneficial heterologous non-specific effects and innate immune memory training through epigenetic reprogramming.5,6 Furthermore secretion of pro-inflammatory cytokines, specifically IL-1B play a vital role in antiviral immunity this is believed to be increased by intradermal inoculation of live attenuated mycobacterium Bovis through BCG vaccine.7
Currently, two clinical trials are ongoing to determine if BCG vaccination protects healthcare workers during the COVID-19 pandemic8.
Review by WHO’s Strategic Advisory Group of Experts on Immunization (SAGE) on nonspecific effects of BCG vaccine shows that vaccination at birth reduces neonatal mortality by 48% (18–67%), which is mainly due to the prevention of neonatal sepsis and respiratory infections9.
Variances in covid 19 incidence and mortality across the world led people to look for possible cause (s).
One thing (among others) is BCG vaccine as far as being subjected to different protocols and policies among different nations. Rapid systematic review and WHO statements regarding vaccine protocols concluded that current evidence does not justify changes to current global immunization policy and they recommend further studies of adequate size and quality to determine the non-specific effects of vaccines on all-cause mortality and findings that show significant correlation between BCG vaccine and COVID-19 provide inadequate evidence and should not be reflected on any practices or policies at the current time, outside the contexts of RCTs.8
These recomondations did not handle the current latent TB protocols variances among nations. Based on the underlying hypotheses of BCG vaccine, I try to look for this from different view which is the beneficial effect of mycobacterium infection through latent infection which carry a natural BCG like effect to the host and reflected indirectly by the prevelance of TB in the community taking in consideration more beneficial effects of latent infection over BCG vaccination as mentioned earlier and I put the question whether variances in prevalence is reflected on covid 19 mortality or not in order to support or reject the BCG and TB prevalence hypotheses.
Material and methods
Data regarding TB prevalence were taken from publically published WHO data while Covid-19 data 2018 were taken from publically published data collected between 30/42/5/2020. Every country has less than 1 million population is excluded also Lebanon is excluded due to recent 1.5 million refugees from Syria.
Total number of sample is 155 Country were put in 5 groups according to BCG criteria shown in table (1)
shows classification of studied sample with ranges of TB prevalence and covid-19 mortality.
statistical Methods:
(Linear and Non-Linear Regression) of predicted equations models, such as (logarithmic, inverse, quadratic, compound, power, s-shape, growth, exponential, and logistic) as well as simple linear regression model with their estimates such that (slope, constant, correlation coefficient, and analysis of variance for regression) are suggested for studying influence of TB prevalence / 100000 in relative to covid-19 mortality / million and as illustrated in the following table (2).
Suggested Predicated Equations for studying the Influence of Tb Prevalence / 100000 in relative to Covid - 19 Mortality / Million
Results
1-Influence of TB prevalence/100000 on covid - 19 mortality/million on (no vaccination at all no previous BCG) group of countries
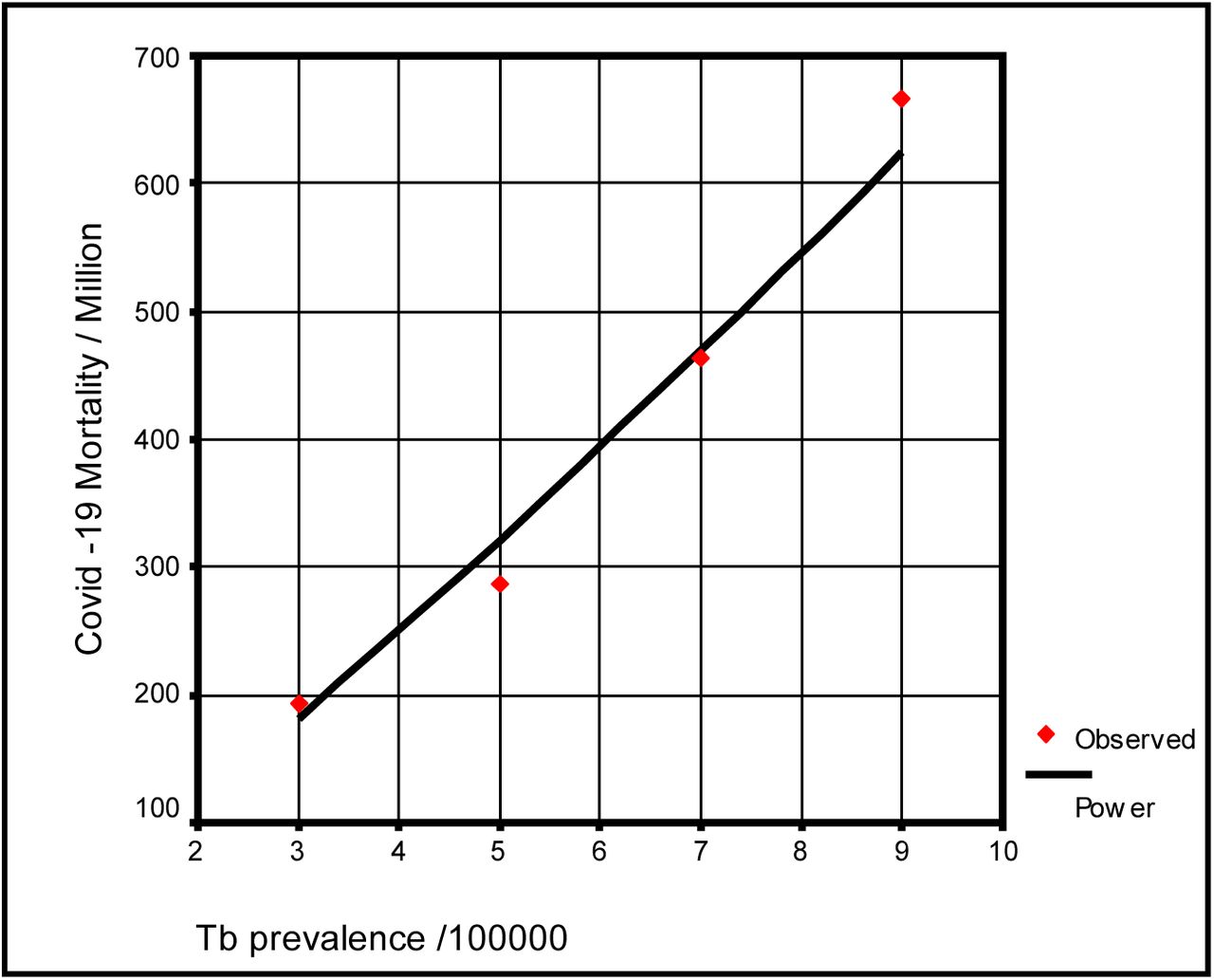
Table (2) shows meaningful nonlinear regression of (Compound model) tested in two tailed alternative statistical hypotheses for two factors, TB Prevalence / 100000 in relation to Covid-19 Mortality / Million for tgroup. Slope value indicates that with increasing one unit of the first factor, occurrence positive influence on unit of the second factor, and estimated by (1.128). The increment recorded significant influence at P<0.05, as well as relationship coefficient at P<0.05 are accounted (0.987) with extremely perfect meaningful determination coefficient (i.e. R-Square = 97.45%). Other source of variations are not included in model, i.e. "Constant term in regression equation" shows that non assignable factors that not included in the regression equation, ought to be informative, since estimated (52) cases of covid - 19 mortality / million expected initially without effectiveness by the restricted of no vaccination at all no previous BCG, with highly significant at P<0.05, which indicates that rather than meaningful and significant relationship between studied factors, a meaningful and highly significant effectiveness of others factors are not included in the predicted model on occurrences of covid-19 mortality / million for (no vaccination at all no previous BCG) group countries.
Influence of TB prevalence / 100000 factor on covid-19 mortality / million factor of no vaccination at all no previous BCG group
Figure (1) shows the long term trend of scatter diagram influence of TB prevalence / 100000 in relative to covid-19 mortality / million for no vaccination at all no previous BCG group.

Long term trend of scatter diagram influence of TB prevalence /100000 with covid-19 mortality/million for no vaccination at all no previous BCG group
2-Influence of TB prevalence/100000 on covid-19 mortality/million on (no current but had BCG in past (one or more)) group of countries
Table (4) shows meaningful nonlinear regression of (Cubic model) tested in two tailed alternative statistical hypotheses for two factors, TB Prevalence / 100000 in relative to Covid-19 Mortality / Million of no current but had 1 BCG in past or more. Slopes values are estimated and indicates that with increasing one unit of the first factor, there is high increments with the second factor up to marginal of 9 TB prevalence rate influence and then decreasing behavior with leftover of the second factor, and recorded high significant influence at P<0.01, as well as relationship coefficient at P<0.01 is accounted (0.81301) with extremely perfect meaningful determination coefficient (i.e. R-Square = 66.098%). Others source of variations that are not included in model, i.e. "Constant term in regression equation" shows that non assignable factors that are not included in the regression equation, ought to be informative, with a high significance at P<0.01, which indicates that rather than meaningful and significant relationship between studied factors, a meaningful and highly significant effectiveness of other factors are not included in the predicted model on occurrences of covid-19 mortality / million of no current but had 1 BCG in past or moregroup.
Influence of TB prevalence / 100000 factor on covid-19 mortality / million factor of no current but had BCG in past or more
Figure (2) shows the long term trend of scatter diagram influence of TB prevalence / 100000 in relative to covid-19 mortality / million for no current but had 1BCG in past or more group.

Long term trend of scatter diagram influence of TB prevalence /100000 with covid 19 mortality/million for no current but had bCg in past or more group
3-Influence of TB prevalence/100000 on covid-19 mortality/million on 1 current BCG and previous booster (s) group of countries
Table (5) shows meaningful nonlinear regression of (Inverse model) tested in two tailed alternative statistical hypothesis of two factors, TB Prevalence / 100000 in relative to covid-19 mortality / Million of 1 current BCG with previous booster (s). Slope value indicates increasing one unit of the first factor, there is a reverse influence on the unit of the second factor, and estimated as (465), and that recorded increment is highly significant at P<0.01, as well as relationship coefficient at P<0.01 are recorded between studied factors, and accounted (0.63662) with meaningful determination coefficient (i.e. R-Square). Other source of variations are not included in model, i.e. "Constant term in regression equation" shows that non assignable factors that not included in the regression equation, could be neglected, since estimated (−1.202066) cases of covid-19 mortality / million expected initially without effectiveness by the g of 1 group current BCG with previous booster (s) group, with no significant at P>0.05.
Influence of TB prevalence / 100000 factor on covid-19 mortality / Million factor of 1 current BCG + previous booster (s)
Figure (3) shows the long term trend of scatter diagram influence of TB prevalence / 100000 in relative to covid-19 mortality / million of 1 current BCG with previous booster (s).

Long term trend of scatter diagram influence of TB prevalence /100000 with covid 19 mortality million for 1 current BCG with previous booster (s) group
4-Influence of TB Prevalence/100000 on covid-19 mortality/million on just 1 BCG now no previous booster (s) group
Table (6) shows meaningful non linear regression of (Logarithm model) tested in two tailed alternative statistical hypothesis of two factors, Tb Prevalence / 100000 in relative to Covid-19 Mortality / Million of just (1) BCG now no previous booster(s). Slope value estimated and indicating that with increasing one unit of the first factor, occurrence negative influence on unit of the second factor, and estimated by (−2.513626), and that increment recorded highly significant and reverse influence at P<0.01, as well as relationship coefficient at P<0.01 are recorded between studied factors, and accounted (0.30751) with meaningful determination coefficient (i.e. R-Square). Others source of variations are not included in model, i.e. "Constant term in regression equation" shows that non assignable factors that not included in the regression equation, ought to be informative, since estimated about (16) cases of Covid-19 Mortality / Million expected initially without effectiveness by the restricted of just (1) BCG now no previous booster(s), with highly significant at P<0.01, which indicates that rather than meaningful and significant relationship between studied factors, a meaningful and high significant effectiveness of others factors are not included in the predicted model on occurrences of covid-19 mortality / million.
Influence of TB prevalence / 100000 factor on covid-19 mortality / million factor of just 1 BCG now no previous booster (s) group
Figure (4) shows the long term trend of scatter diagram influence of TB prevalence / 100000 in relative to covid-19 mortality / million of just (1) BCG now no previous booster(s).

Long term trend of scatter diagram influence of TB prevalence /100000 with covide-19 mortality/million of just 1 BCG now, no previous booster (s)group
5-Influence of TB Prevalence/100000 on Covid-19 Mortality/Million on more than (1 BCG setting now) group countries
Table (7) shows meaningful nonlinear regression of (Inverse model) tested in two tailed alternative statistical hypothesis of two factors, TB Prevalence / 100000 in relative to Covid-19 Mortality / Million of more than 1 BCG setting now. Slope value indicates that with increase one unit of the first factor, there is a reverse influence on the unit of the second factor, and estimated by (138), and that increment recorded significant at P<0.05, as well as relationship coefficient at P<0.05 are recorded between studied factors, and is accounted (0.61580) with meaningful determination coefficient (i.e. R-Square). Other source of variations are not included in model, i.e. "Constant term in regression equation" shows that non assignable factors that not included in the regression equation, could be neglected, since estimated (7.555379) cases of covid-19 mortality / million expected initially without effectiveness by the group more than 1 BCG setting now, with no significant at P>0.05.
Influence of Tb Prevalence / 100000 factor on Covid-19 Mortality / Million factor of more than 1 BCG setting now
Figure (5) shows the long term trend of scatter diagram influence of Tb Prevalence /100000 in relative to Covid-19 Mortality / Million of more than 1 BCG setting now.

Long term trend of scatter diagram influence of Tb prevalence /100000 with covide 19 mortality/million of more than 1 BCG setting now
6-Influence of Tb Prevalence/100000 on covid-19 mortality/million on overall countries
Table (8) shows meaningful nonlinear regression of (Logarithm model) tested in two tailed alternative statistical hypothesis of two factors, TB prevalence / 100000 in relative to covid-19 mortality / million of an overall restricted of BCG status. Slope value indicates that with increasing one unit of the first factor, there is negative influence on unit of the second factor, and estimated by (−23.49066), and that increment recorded as highly significant with reverse influence at P<0.01, as well as highly significant relationship coefficient at P<0.01 is recorded between studied factors, and accounted (0.36749) with meaningful determination coefficient (i.e. R-Square). Other source of variations not included in studied model, i.e. "Constant term in regression equation" shows that non assignable factors that are not included in the regression equation, ought to be informative, since estimated (122) cases of covid-19 mortality / million expected initially without effectiveness by the restricted of just (1) BCG now no previous booster(s), with highly significant at P<0.01, which indicates that rather than meaningful and significant relationship between studied factors, a meaningful and high significant effectiveness of others factors are not included in the predicted model on occurrences of Covid-19 Mortality / Million.
Influence of TB prevalence / 100000 factor on covid-19 mortality / million factor of an overall groups
Figure (6) shows the long term trend of scatter diagram influence of TB prevalence / 100000 in relation to covid-19 mortality / million overall groups.

Long term trend of scatter diagram influence of TB prevalence /100000 with covid-19 mortality/million of an overall groups.
Discussion
Lebanon about 6.830 million was excluded due recent 1.5 million refugees from Syria and 400,000 Palestinian refugees in addition to 1 million foreign workers (mainly Syrians) and there is a sizeable Lebanese diaspora. Countries with just thousands of people up to less than 1 million populations are excluded because it impossible to look for 1 million mortalities for covid 19 unless adjusting figures by augmenting population figures.
Our data suggest that TB prevalence seems to significantly reversely associated with reduction in mortality associated with covide-19 this finding is enhanced by BCG status being the more frequent the vaccine given the less covid-19mortality is. As far as active TB infection reflects 10 % iceberg of total TB infection, latent TB possibly works with same mechanism that BCG works in provocation immunity towards viruses. Strong association in this study might reflect a more potent effect of prevalence over BCG.
The strong negative association between covid-19 mortality and TB prevalence in many tables is going parallel with underling hypotheses of our study and furtherly support BCG theory which was tested many weeks before.
Significant inverse and logarithmic associations among tablets reflect augmentation effect of vaccination and possibly effect of revaccination these finding support the previously mentioned hypotheses by different way and may raise the question of early interventions before clinical control trials result proceed, specially these trials will take a time while urgent actions are needed to contain the disease in context of available evidence at this time. The possible actions according to this study include questioning BCG practices as previous studies recommends and extends to policies whether to treat latent TB infections or not specially the WHO recommends tailored latent tuberculosis infection management based on tuberculosis burden and resource availability10. These make these recommendations wider than previous BCG studies in this aspect although it is based on the same underling hypotheses.
Treatment of latent TB to prevent about 5 to 10 percent of infected people who will develop TB disease if not treated is a common practice in developed countries 11 and this should be reevaluated.
Tuberculosis Prevalence is defined as the number of TB cases (all forms) at a given point in time12. and an algorithm for excluding active tuberculosis was specified in the policies of 43 (63.2%) low-burden countries13. The content of that algorithm varied greatly from country to country. In Ecuador the recommendation was only that active tuberculosis should be ruled out, with no mention of an exclusion algorithm.13 Furthermore recorded HIV prevalence is highest in Ecuador at 35% this might explains the high prevalence rate of TB and unproportioned covid-19 mortality due to possible inclusion of latent Tb in prevalence of TB due to high HIV in absence of inclusion criteria regarding absent of exclusion algorithm.
In 2014, the global burden of LTBI was 23.0%, amounting to approximately 1.7 billion people. WHO South-East Asia, Western-Pacific, and Africa regions had the highest prevalence and accounted for around 80% of those with LTBI14. On the country level, China and India had the highest LTBI burden, approximately 350 million infections, followed by Indonesia at around 120 million infections and fewer than 60 million infections in all other countries. The USA had the 20th burden, at an estimated 13 million.14 the diversity of spread and mortality goes parallel with low latent TB places and supported by low prevalence of TB according to this study.
Conclusion: TB prevalence is strongly associated with covid-19 mortality and being more sever in absence of BCG vaccine.
Data Availability
All data referred to in the manuscript are available on requist
Recommendations
Randomized clinical trials are recommened on this aspect.
Early interventions might be considered based on the supportive evidence at this time which include BCG vaccination protocols and review of current latent TB programs.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}