
Abstract
Coronavirus disease 2019 (COVID-19) is a global pandemic and has been widely reported; however, a comprehensive systemic review and meta-analysis has not been conducted. We systematically investigated the clinical characteristics of COVID-19 in mainland China to guide diagnosis and treatment. We searched the PubMed, Embase, Scopus, Web of Science, Cochrane Library, bioRxiv, medRxiv, and SSRN databases for studies related to COVID-19 published or preprinted in English or Chinese from January 1 to March 15, 2020. Clinical studies on COVID-19 performed in mainland China were included. We collected primary outcomes including signs and symptoms, chest CT imaging, laboratory tests, and treatments. Study selection, data extraction, and risk of bias assessment were performed by two independent reviewers. Qualitative and quantitative synthesis was conducted, and random-effects models were applied to pooled estimates. This study is registered with PROSPERO (number CRD42020171606). Of the 3624 records identified, 147 studies (20,662 patients) were analyzed. The mean age of patients with COVID-19 was 49.40 years, 53.45% were male, and 38.52% had at least one comorbidity. Fever and cough were the most common symptoms, followed by fatigue, expectoration, and shortness of breath. Most patients with COVID-19 had abnormal chest CT findings with ground glass opacity (70.70%) or consolidation (29.91%). Laboratory findings shown lymphopenia, increased lactate dehydrogenase, increased infection-related indicators, and fibrinolytic hyperactivity. Antiviral therapy, antibiotic therapy, and corticosteroids were administered to 89.75%, 79.13%, and 35.64% of patients, respectively. Most clinical characteristics of COVID-19 are non-specific. Patients with suspected should be evaluated by virological assays and clinically treated.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the seventh human coronavirus identified, with bats thought to be the original host.1-3 SARS-CoV-2 is approximately 50% genetically identical to Middle East respiratory syndrome coronavirus (MERS-CoV) and approximately 79% identical to severe acute respiratory syndrome coronavirus (SARS-CoV) and shows a similar receptor-binding domain structure.4 Patients infected with SARS-CoV-2 may be asymptomatic or have mild to severe pneumonia. The syndrome of clinical symptoms caused by SARS-CoV-2 is named as coronavirus disease 2019 (COVID-19).5
COVID-19 is the third type of zoonotic coronavirus disease after SARS and MERS occurring in the last two decades. COVID-19 is highly contagious through respiratory droplets and contact and has caused global pandemic. As of April 17, 2020, COVID-19 has spread to 213 countries and regions globally, causing 2,074,529 confirmed cases and 139,378 deaths.6 At present, the United States and Europe have become the hardest-hit regions by COVID-19, with 632,781 confirmed cases in the United States of America, 1,050,871 confirmed cases in European region.
Governments worldwide must urgently need to learn from China’s experience, as China experienced a rapid growth period followed by a stable decline period of the COVID-19 epidemic, and currently a recovery period.
Since the outbreak of COVID-19, a large number of articles have been published or preprinted reporting its epidemiologic and clinical characteristics. However, few large studies have been reported, and variations in reporting descriptive data may lead to the misunderstanding of the clinical features of COVID-19. In this review, we systematically investigated the epidemiologic, characteristics, chest computed tomography (CT) imaging, laboratory findings, and treatments of COVID-19 in mainland China. Our findings provide important guidance on the diagnosis and treatment of the current global COVID-19 pandemic.
Methods
Search strategy and selection criteria
For this systematic review and a meta-analysis, we searched the PubMed, Embase, Scopus, Web of Science, Cochrane Library, bioRxiv, medRxiv, and SSRN electronic databases for papers published or preprinted in English or Chinese from January 1 to March 15, 2020 with the following search terms: “coronavirus disease 2019” OR “COVID-19” OR “SARS-CoV-2” OR “2019-nCoV” OR “Novel Coronavirus” OR “Wuhan pneumonia”. Additional studies were identified by manually searching the reference lists of primary studies and review articles. The authors of full papers were contacted for additional information when required.
The inclusion criteria were as follows: clinical studies of COVID-19; studies performed in mainland China; number of cases ≥10; and primary outcomes including signs and symptoms, chest CT imaging, laboratory tests, and treatments were available. We excluded studies conducted outside of China; case reports, case series, reviews, abstract, and opinions; those without primary outcomes.
Two investigators (CT, KZ) independently reviewed the title and abstract of the retrieved articles to select eligible articles according to the inclusion criteria. After excluding duplicated and irrelevant studies, the full-text of the remaining studies was reviewed to assess the eligibility for inclusion. The inter-rater agreement of study selection was measured using the κ statistic. If multiple studies used the same dataset or cohort, we included the most comprehensive study with the largest number of participants and excluded the others. Disagreements were resolved by consensus or were arbitrated by a third investigator (ZL).
Data analysis
Two investigators (CT, WW) independently extracted primary and secondary outcomes from the eligible studies using a predefined and standardized data extraction checklist, with disagreements resolved by discussion. The following information were recorded: first author, province, city, sample size, gender, age, smoker, comorbidities, symptoms, chest CT imaging, laboratory findings, complications, treatments, and prognosis. For missing data, we evaluated online supplementary appendixes or contacted the first or corresponding author to obtain the missing data or more information. If no response was obtained, we calculated the data using methods such as imputing the mean and standard deviation (SD) from the median, interquartile range (IQR), and full range as described by Wan et al.7 and Luo et al.8
Two investigators (ZP, PY) independently assessed the risk of bias in the eligible studies, with disagreements resolved through discussion. The Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) was used to assess study quality.9 ROBINS-I contains seven domains: (1) bias due to confounding factors; (2) bias in the selection of participants for the study; (3) bias in classification of interventions; (4) bias due to deviations from the intended interventions; (5) bias due to missing data; (6) bias in the measurement of outcomes; and (7) bias in the selection of reported results. The categories for risk of bias judgement were “Low risk”, “Moderate risk”, “Serious risk”, “Critical risk”, and “No information”, with a high-quality study defined as one showing a “Low risk” or “Moderate risk”. Studies were excluded when the quality was “Critical risk” or “No information”.
R version 3.6.2 and Stata version 15 (StatCorp, College Station, TX, USA) were used for statistical analyses. All data are expressed as overall summary estimates and 95% confidence intervals (CIs). Cochran’s Q test and I2 statistic were used to assess heterogeneity, with p < 0.05 for Cochran’s Q test or I2 >50% indicating significant heterogeneity, in which cases the random-effects model was used. Otherwise, the fixed-effects model was used. Heterogeneity was assessed by meta-regression of province, sample size, and age. Potential publication bias was assessed by quantitative Egger’s linear regression test. This study is registered with PROSPERO (number CRD42020171606).
Results
A total of 3624 records were retrieved, after removing the duplicates, 2751 records were retained. We screened the titles and abstracts and excluded 2493 ineligible records. The full-texts of the remaining 258 records were assessed for eligibility, of which 111 were excluded. Of the selected 147 articles, 143 were written in English and 4 were in Chinese. The study selection flow is shown in Figure 1 and the characteristics on eligible articles is shown in Table 1.
Characteristics of included studies

The results of quality assessment of the included studies are shown in the appendix (pp 2-7). Overall, 117 high-quality studies and 30 fair-quality studies were included in the meta-analysis.
Epidemiology and comorbidities of COVID-19
A total of 20,662 patients with COVID-19 were included. Patient ages ranged from 1 month to 100 years old, with a mean age of 49.40 years (95%CI of 45.15–53.65 years). The proportion of males was 53.45% (95%CI 52.02–54.92%). Among 5094 patients in 35 studies, 511 were smokers, accounting for 9.93% of patients (95%CI 7.87–12.54%).
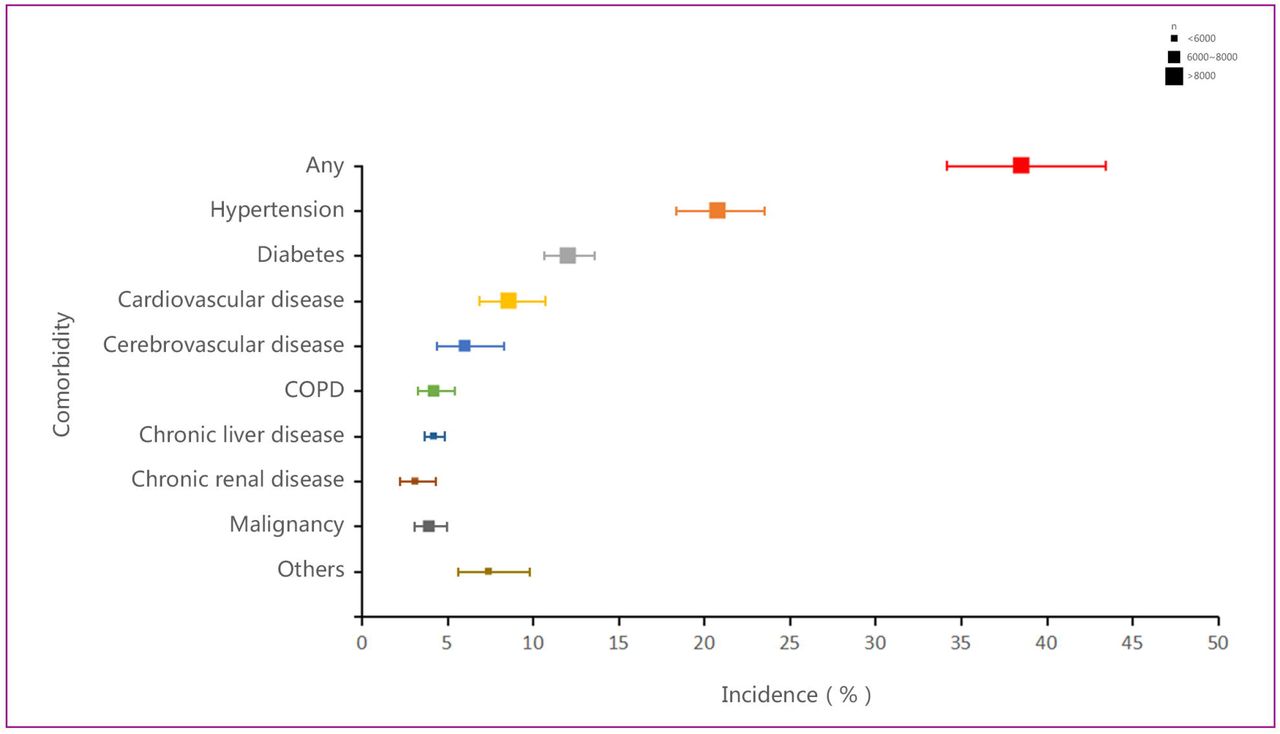
Of 8028 patients with COVID-19, 3066 (38.52%, 95%CI 34.17–43.42%) had at least one comorbidity, including hypertension (20.78%), diabetes (12.04%), cardiovascular disease (8.58%), cerebrovascular diseases (6.01%), chronic obstructive pulmonary disease (4.20%), chronic liver disease (4.19%), malignancy (3.92%), and chronic renal disease (3.11%). (see Figure 2, Appendix pp 8)

Note: COPD= chronic obstructive pulmonary disease.
Signs and symptoms of COVID-19
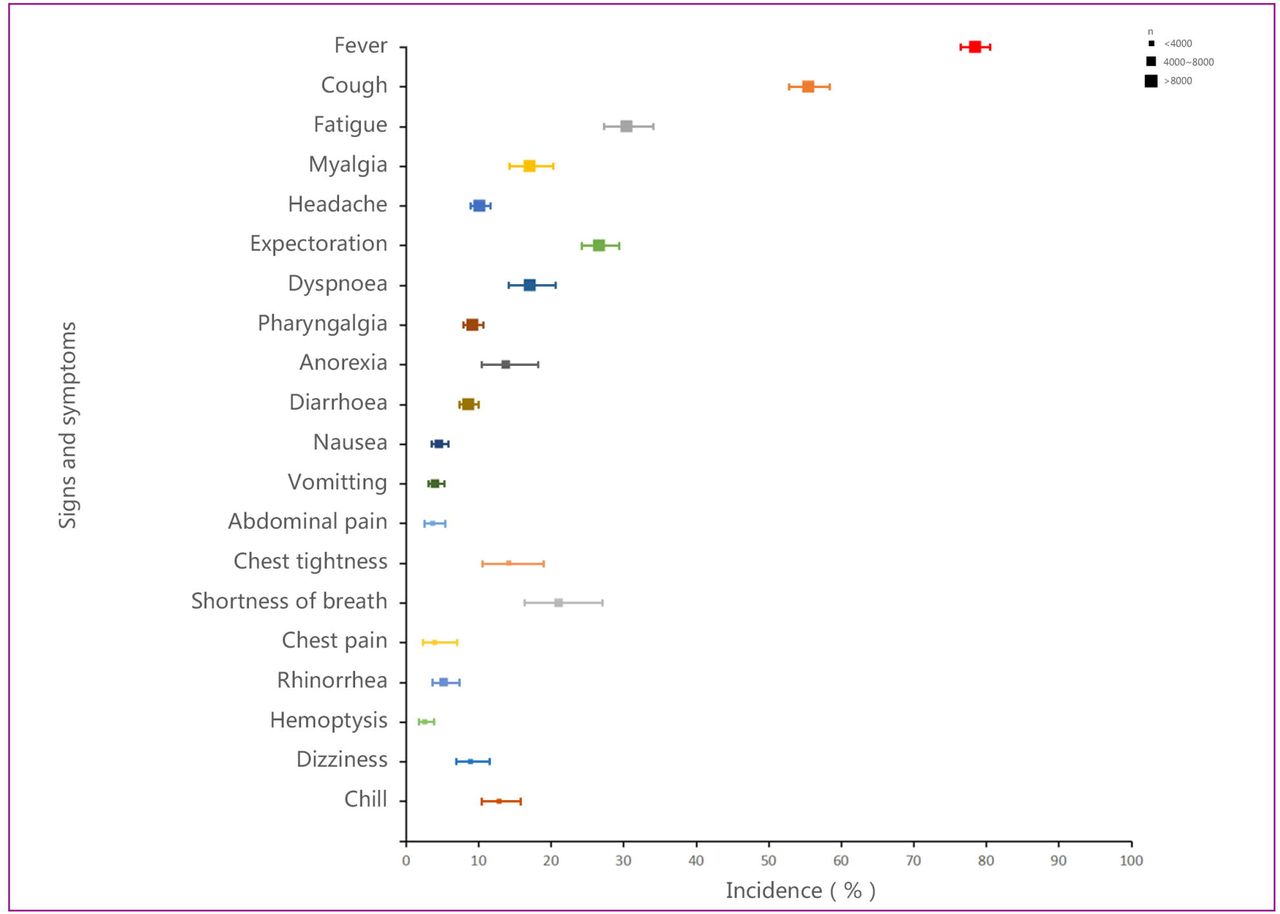
The most common symptom of COVID-19 was fever. Of 18,513 patients with COVID-19, 13,707 (78.49%, 95%CI 76.47–80.56%) had fever. The proportions of patients with mild to moderate fever were 30.96% and 35.02%, and only 11.45% of patients had high fever. Patients also experienced cough (55.49%, 95%CI 52.71–58.41%), fatigue (30.42%, 95%CI 27.20–34.03%), expectoration (26.64%, 95%CI 24.13–29.41%), shortness of breath (21.07%, 95%CI 16.33–27.17%), dyspnea (17.08%, 85%CI 14.15–20.60%), myalgia (17.06%, 95%CI 14.32–20.32%), chest tightness (14.19%, 95%CI 10.61–18.98%), anorexia (13.78%, 95%CI 10.42–18.21%), chill (12.86%, 95%CI 10.47–15.79%), and headache (10.14%, 95%CI 8.84–11.63%). Less common symptoms were pharyngalgia (9.17%), dizziness (8.92%), diarrhea (8.61%), rhinorrhea (5.21%), nausea (4.56%), vomiting (4.02%), chest pain (3.98%), abdominal pain (3.71%), and hemoptysis (2.62%). (see Figure 3, Appendix pp8-9)

CT imaging and laboratory findings of COVID-19
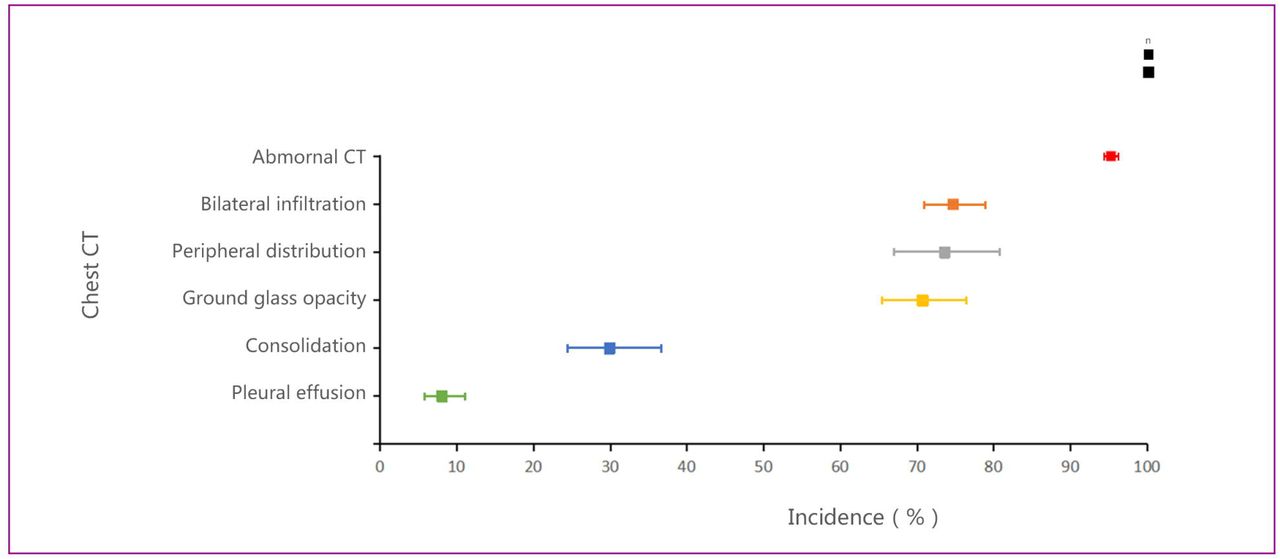
Of 8711 patients with COVID-19, 7919 (95.31%) had abnormal presentations on chest CT imaging, with 74.72% bilateral infiltration, 73.60% peripheral distribution, 70.70% ground glass opacity, 29.91% consolidation, and 8.06% pleural effusion. (Figure 4, Appendix pp 9)

The mean values for the leucocyte count, neutrophil count, lymphocyte count, platelet count, and hemoglobin were all in the normal range. The proportion of patients with increased leukocytes and neutrophils were 10.55% and 4.05%, respectively, whereas those with decreased leukocytes, neutrophils, lymphocytes, platelets, and hemoglobin were 24.26%, 16.64%, 48.20%, 5.80%, and 23.56%, respectively.
The mean values for albumin, alanine transaminase (ALT), aspartate transaminase (AST), total bilirubin (TB), blood urea nitrogen (BUN), serum creatinine (SCr), creatine kinase (CK), and creatine kinase-MB (CK-MB) were all in the normal range. The mean value for lactate dehydrogenase (LDH) was moderately elevated to 308.76 U/L (95%CI 264.28–353.24 U/L). The proportion of patients showing decreased albumin was 37.51%, whereas the proportion of patients showing increased for ALT, AST, TB, BUN, SCr, LDH, CK, and CK-MB were 19.02%, 23.61%, 9.48%, 12.71%, 7.21%, 41.55%, 13.87%, and 16.76%, respectively. The mean values for potassium and sodium were in the normal range.
The mean values for activated partial thromboplastin time (APTT), prothrombin time (PT), D-Dimer, and fibrinogen were in the normal range. The proportion of patients showing increased APTT, PT, D-Dimer, and fibrinogen were 25.60%, 15.78%, 43.33%, and 36.90%, respectively.
Infection-related indicators including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), interleukin-6 (IL-6), and serum ferritin (SF) were all increased, with mean values of 32.05 mg/L (95%CI 27.34–36.75 mg/L), 36.37 mm/h (95%CI 30.53–42.21 mm/h), 13.90 pg/mL (11.53–16.26 pg/mL), and 714.73 ng/mL (95%CI 568.92–860.55ng/mL), respectively. Only procalcitonin (PCT) was in the normal range. The proportion of patients with increased CRP PCT, ESR, IL-6, and SF were 61.59%, 17.23%, 62.90%, 57.33%, and 76.47%, respectively. (Figure 5, Appendix pp 9-11)

Complications and treatments of COVID-19
Common complications of COVID-19 included acute respiratory distress syndrome (ARDS) (25.09% 95%CI 18.88–3.35%), acute liver injury (21.68%, 95%CI 14.65–32.08%), secondary infection (17.14%, 95%CI 10.72–27.41%), acute cardiac injury (10.61%, 95%CI 7.20–15.64%), acute kidney injury (7.12%, 95%CI 4.74–10.70%), and shock (6.05%, 95%CI 3.09–11.85%). (see Figure 6, Appendix pp 12)

Of 7510 COVID-19 patients, 5988 (89.75%, 95%CI 87.90–91.64%) were administered antiviral therapy, 79.13% with antibiotic therapy, 35.64% with corticosteroids, 31.69% with immunoglobulin, and 71.07% with γ-interferon. Additionally, 3073 of 5703 cases (61.91%) were administered oxygen support, 14.52% with non-invasive mechanical ventilation, and 7.48% with invasive mechanical ventilation. Sixty-two of 4012 cases (2.27%) were administered extracorporeal membrane oxygenation and 74 of 1656 cases (4.47%) were administered continuous renal replacement therapy. Further, 14.87% of patients with COVID-19 were admitted to the intensive care unit and 6262 patients reported clinical outcomes. There were 3664 hospitalizations; 2133 patients improved and were discharged, and 233 patients died. Mortality was 3.09% (1.85–5.15). (see Figure 7, Appendix 11-12)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
In this review, we retrospectively analyzed clinical data from patients with COVID-19. These patients were admitted to hospitals between December 2019 and February 2020, which covered the rapid growth period of the COVID-19 epidemic in mainland China. This meta-analysis is the first comprehensive summary of the clinical characteristics of COVID-19 in mainland China. Through literature retrieval and data extraction, we identified 20,662 patients confirmed to have COVID-19 reported in 147 articles. The patients ranged in age from 1 month to 100 years old, with a mean age was 49.40 years, which is consistent with a China CDC report.157 This suggests that the general population, regardless of age, is susceptible to SARS-CoV-2 infection. In addition, some studies suggested that advanced age is a risk factor for severe illness and mortality.15,19,90,92 The proportion of males was 53.45%, indicating that COVID-19 does not have a gender predisposition. Approximately 1 in 10 patients had a history of smoking, but whether this population was more susceptible to COVID-19 remains unclear. Of 8028 COVID-19 patients, 38.52% had at least one comorbidity, most commonly hypertension and diabetes. Any comorbidity is an important factor in poor prognosis. Patients with hypertension, diabetes, and cardiovascular and cerebrovascular diseases are at a higher risk of severe illness or death.19,90
We also summarized 20 clinical symptoms. The most common symptom observed in patients with COVID-19 was fever; approximately two-thirds of patients had mild to moderate fever, whereas only 11.45% of patients had high fever. The second most common symptom was cough, and approximately one-quarter of COVID-19 patients produced sputum. Because angiotensin-converting enzyme 2 of alveolar epithelial cells is the receptor for SARS-CoV-2,158 this infection induced excessive host immune responses, causing diffuse alveolar damage and lymphocytic infiltration in both lungs,159 manifested as dyspnea and shortness of breath. However, patients with COVID-19 rarely showed obvious signs and symptoms in the upper respiratory tract (pharyngalgia, rhinorrhea, nasal obstruction). Fatigue and myalgia were the most common musculoskeletal symptoms. In addition, gastrointestinal symptoms such as anorexia, diarrhea, nausea, vomiting, and abdominal pain were rare in patients with COVID-19. Thus, fever and cough are the most typical clinical symptoms.
In our study, most patients with COVID-19 had abnormal findings in chest CT imaging. The typical CT findings were characterized by ground glass opacity or consolidation. In addition, bilateral lungs infiltration and peripheral distribution were consistent with the pathological findings.159 According to the Guidelines for the Diagnosis and Treatment of Novel Coronavirus Infection, clinical diagnosis can be made by typical chest CT imaging, particularly when nucleic acid assays are scarce.160 In laboratory tests, the mean values of blood routine and biochemistry parameters were in the normal range. Nearly one-half of patients with COVID-19 had lymphocytopenia, and about a quarter of patients had leukopenia and anemia. Because angiotensin-converting enzyme 2 is widespread in the heart and liver, LDH was moderately elevated, and the proportion of patients showing increased for ALT, AST, CK, and CK-MB were 19.02%, 23.61%,13.87% and 16.76%, respectively. However, indicators of kidney function such as blood urea nitrogen, serum creatinine were not obviously elevated. In addition, the proportions of D-Dimer and fibrinogen were increased, suggesting that patients with COVID-19 had a fibrinolytic hyperactivity status. Infection-related indicators in patients with COVID-19 were generally increased, including the C-reactive protein, erythrocyte sedimentation rate, interleukin-6, and serum ferritin, suggesting the presence of an inflammatory storm or secondary infection in these patients. According to Wang et al.,19 patients with severe ill are more prone to laboratory abnormalities, including increased leukocytes, decreased lymphocytes, abnormal liver function, abnormal coagulation function, and increased infection-related indicators, leading to ARDS, acute myocardial injury, acute liver injury, and shock. Lymphocytopenia, increased LDH, increased D-dimer, and increased infection-related indicators, particularly IL-6, have been suggested to lead to a poor prognosis.90,92
Most patients with COVID-19 were administered antiviral therapy such as oseltamivir or lopinavir,30,161 whereas a large percentage of patients were administered γ-interferon as an anti-viral agent to improve immunity. Antibiotic therapy was used in most patients to treat secondary infection or sepsis. Additionally, anti-inflammatory treatment was essential because of the cytokine storm;162 more than one-third of patients were administered systemic corticosteroids. However, caution should be used when administering corticosteroids therapy avoid side-effects such as weakened immunity, nosocomial infections, psychosis, diabetes, and avascular necrosis.163 Only 233 deaths occurred among 6262 COVID-19 patients; the mortality rate was 3.09% consistent with data from the World Health Organization.6
This study had both strengths and limitations. This meta-analysis is the most comprehensive assessment and robust evidence to date of the clinical characteristics of patients with COVID-19 in mainland China. We evaluated 147 published and preprinted studies involving 20,662 patients, equivalent to a quarter of all confirmed cases in mainland China and reflecting the clinical characteristics of patients with COVID-19.6 There were some limitations to our study. First, this study was retrospective, and most studies were preprinted articles that had not been peer-reviewed, leading to a moderate overall quality of the literature. Second, not all clinical characteristics were well-documented, such as chest CT or laboratory tests, leading to inconsistencies in the total number of each item calculated. This also led to heterogeneity. Third, all included cases were treated from December 2019 to February 2020, and many were reported by several hospitals in Wuhan, Hubei province. There may be repeated reports of some cases, leading to a significant heterogeneity and obvious publication bias. To overcome these issues, we used random effects for meta-analysis, meta-regression tests, and Egger’s test. Finally, we were unable to determine the incubation period of COVID-19 because of the heterogeneity among studies in reporting the timeline of cases.
In summary, COVID-19 is an emerging infectious disease with various clinical manifestations. The morbidity of COVID-19 is not age- and sex-dependent. The most common clinical symptoms were fever (78.49%) and cough (55.49%). Chest CT imaging showed abnormal findings in most patients with ground glass opacity or consolidation around the periphery of the bilateral pulmonary. The main characteristics in laboratory findings were lymphopenia, increased LDH, increased infection-related indicators, and fibrinolytic hyperactivity. Complications such as ARDS and acute liver injury often occur in patients with severe ill. Antiviral therapy, antibiotics, and oxygen support are the most important treatments, and hormone therapy is used in some critical patients. Our findings provide important guidance for the current global pandemic in the diagnosis and treatment of COVID-19.
Data Availability
All data referred to in the manuscript are available. All data in the submitted article.
Contributors
JG, ZG, PY and CT conceived the idea of the study and developed the protocol. CT, KZ and ZL did the literature search and studies selection. CT, WW extracted relevant information. ZP and PY assessed the risk of bias in the eligible studies. CT synthesized the data and wrote the first draft of the manuscript. ZL, PY, ZG and JG revised successive drafts of the paper and approved the final version. ZG supervised the overall work and is the guarantor of the review.
Declaration of interests
We declare no competing interests.
References




